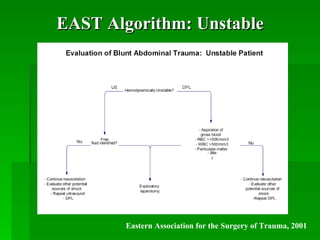
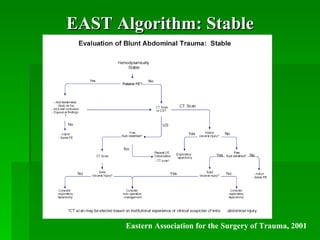
This document summarizes blunt abdominal trauma evaluation. It outlines the anatomy of the abdomen, common injury mechanisms and patterns including injuries to solid organs like the liver and spleen from deceleration forces. Assessment involves history of the traumatic mechanism and physical exam noting signs like abdominal tenderness. Diagnostic tools discussed include labs, plain films, diagnostic peritoneal lavage, focused assessment with sonography for trauma (FAST) exam, and CT scanning. Algorithms are provided for managing unstable versus stable patients based on exam and test findings.