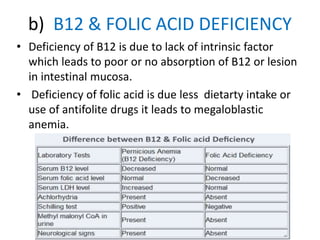
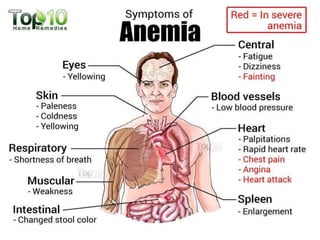
This document defines anemia and classifies it etiologically and morphologically. Anemia is characterized by a decrease in red blood cells (RBCs) or hemoglobin. It grades the severity based on hemoglobin levels. The main etiological classifications are dietary deficiencies like iron deficiency anemia (IDA) and vitamin B12/folic acid deficiency, hemorrhagic anemias, aplastic anemia, and hemolytic anemias. Hemolytic anemias include sickle cell anemia and thalassemias. Morphological classifications depend on RBC size and hemoglobin content, like microcytic hypochromic in IDA. Effects of anemia on the cardiovascular system are also discussed.