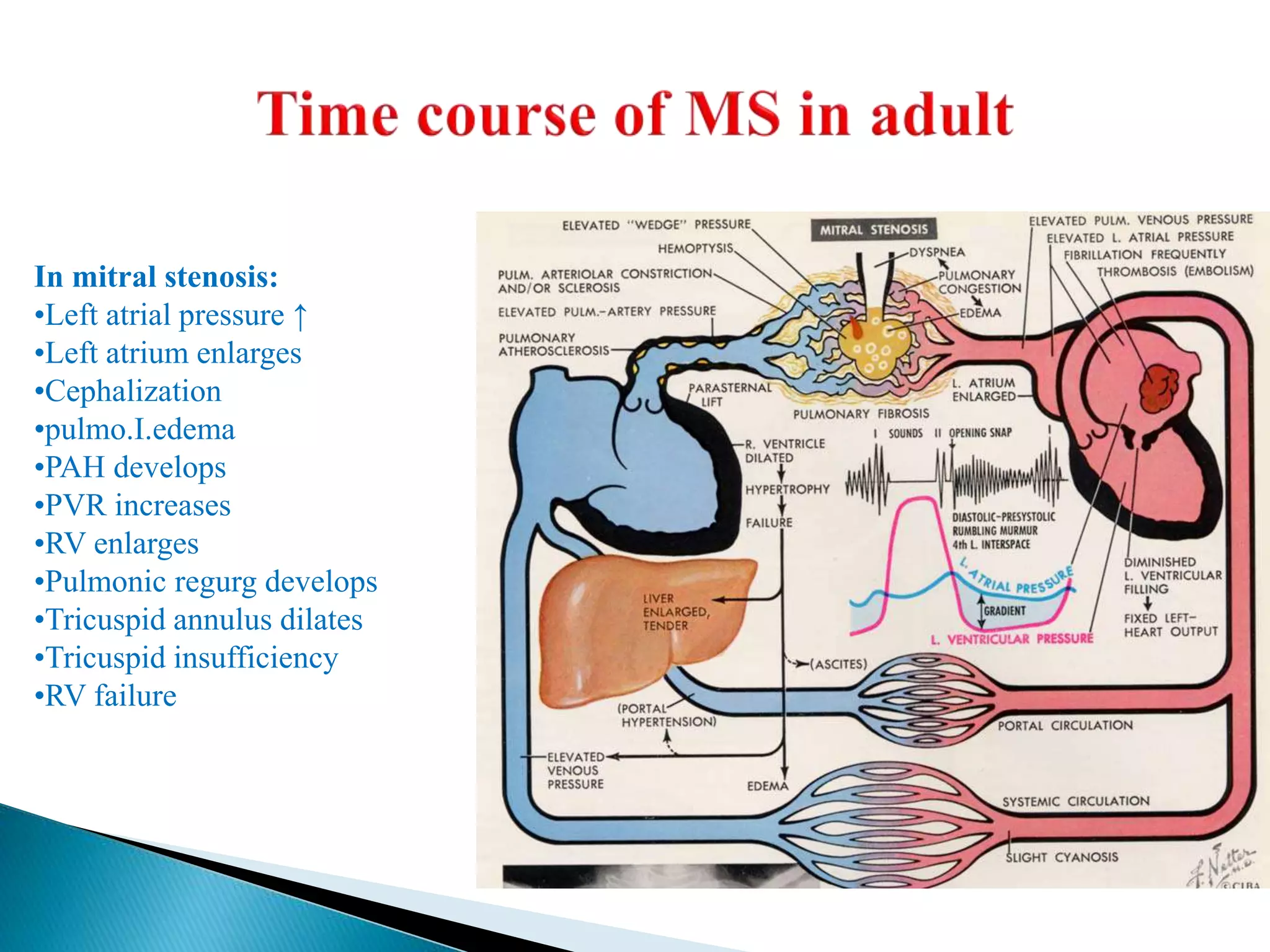
The mitral valve develops between the 5th and 15th weeks of gestation. It consists of an annulus, two leaflets, chordae tendineae and papillary muscles. Rheumatic fever is a leading cause of mitral stenosis, which results from repeated bouts of inflammation damaging the mitral valve over time. Mitral stenosis causes elevated left atrial pressure and left atrial enlargement, often resulting in pulmonary hypertension. Echocardiography is the primary imaging method used to evaluate the mitral valve anatomy and measure the severity of mitral stenosis.