The Mitral Valve
Theleft Atrio-ventricular valve, or bicuspid
valve.
Permits blood flow from the left atrium (LA)
to the left ventricle (LV) during diastole and
sealing of the LA from the LV during
systole.
3.
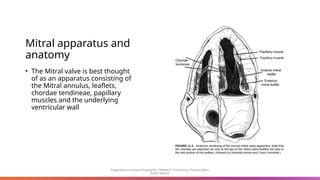
Mitral apparatus and
anatomy
•The Mitral valve is best thought
of as an apparatus consisting of
the Mitral annulus, leaflets,
chordae tendineae, papillary
muscles and the underlying
ventricular wall
Feigenbaum’s echocardiography / William F. Armstrong, Thomas Ryan.
Eighth edition
4.
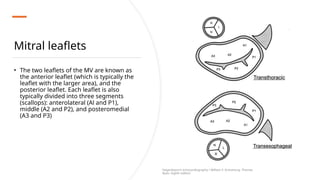
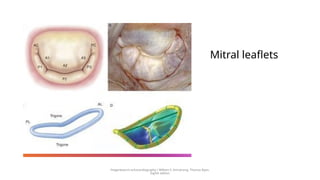
Mitral leaflets
• Thetwo leaflets of the MV are known as
the anterior leaflet (which is typically the
leaflet with the larger area), and the
posterior leaflet. Each leaflet is also
typically divided into three segments
(scallops): anterolateral (Al and P1),
middle (A2 and P2), and posteromedial
(A3 and P3)
Feigenbaum’s echocardiography / William F. Armstrong, Thomas
Ryan. Eighth edition
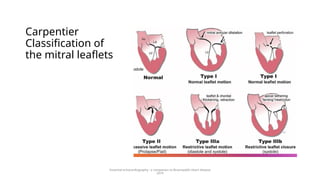
Carpentier
Classification of
the mitral
leaflets
•Mitral anatomy and motion are commonly
defined by the Carpentier classification. This
classification classifies the leaflets as either
normal or abnormal, and furthermore
defines their motion with respect to the
mechanism of mitral regurgitation.
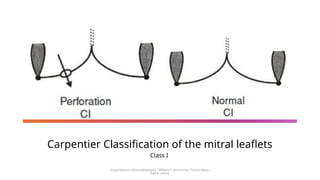
Carpentier class I is defined as normal leaflet
motion in which mitral regurgitation is
functional due to annular dilation or
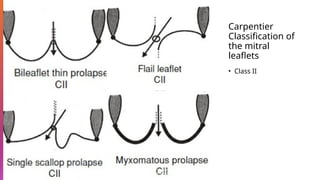
perforation of a mitral leaflet. Class II is
defined as leaflets with prolapse or loss of
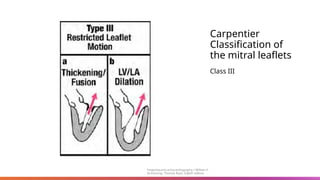
support and excess motion. Carpentier class
III is defined as restricted leaflet motion and
furthermore subdivided into IIIa in which
motion is abnormal in diastole and IIIb in
which it is abnormal in systole
Feigenbaum’s echocardiography / William F. Armstrong, Thomas Ryan.
Eighth edition
7.
Carpentier Classification ofthe mitral leaflets
Class I
Feigenbaum’s echocardiography / William F. Armstrong, Thomas Ryan.
Eighth edition
Mitral Regurgitation
• MRis classically subdivided into two broad categories with
distinct underlying mechanisms: primary MR or secondary MR.
• Primary MR encompasses MV disease in which there is a
structural abnormality of the leaflets and/or associated chords.
• secondary MR, the MV leaflets are essentially normal but the
LV is dysfunctional and distorted due to ischemic or myopathic
remodeling resulting in leaflet tethering and incomplete
closure of the mitral leaflets.
• The differentiation between these types of MVD is necessary
because management, particularly surgical decision making, is
dependent on the underlying etiology of the MV dysfunction
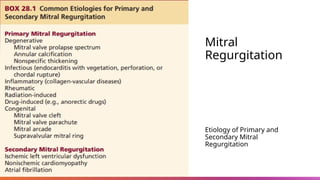
Primary Mitral Regurgitation
•The most common cause of primary MR in developed countries is MV prolapse or flail
(Carpentier type II)
• Prolapse is defined as leaflet billowing by more than 2 mm above the annular “plane” during
systole.
• assessment is typically made in the parasternal long axis view, which displays the highest
points of the saddle-shaped annulus.
• The diagnosis of prolapse should not be made exclusively from the apical four-chamber view,
which shows lower (more apical) points on the annulus.
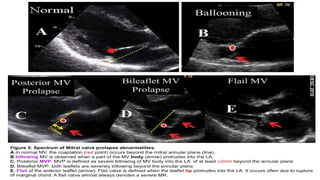
• MV prolapse spans a spectrum from minimum prolapse of the leaflets into the left atrium to
diffuse leaflet thickening and redundancy.
• Flail leaflet is part of the MV prolapse spectrum and is defined as occurring when the leaflet
becomes everted and loses its normal convex shape with the leaflet tip seen within the left
atrium.
• Flail leaflet is caused by disruption of the primary (marginal) chordae such that effective
coaptation is no longer present.
16.
Clinically important MVprolapse/flail
typically presents as two types :
Barlow disease: is an infiltrative disease characterized by
excessive myxomatous tissue associated with
mucopolysaccharide accumulation that can affect one or both
leaflets, and chordae.
In Barlow disease, there is thickening of the leaflets leading to
redundant valvular tissue and frequently elongated or ruptured
chordae.
Patients with Barlow disease are usually diagnosed in young
adulthood and typically present with bileaflet and
multisegmental prolapse with or without flail scallops
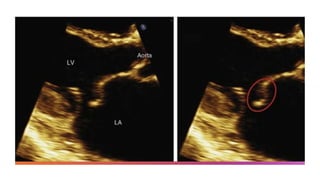
17.
Video Coutresy ofCardiodynamic Athens YouTube cha
nnel
Barlow’s
Disease Echo.
18.
Clinically important MVprolapse/flail
typically presents as two types :
Fibroelastic deficiency, which is the most common form of degenerative
MR in the MV prolapse spectrum, the loss of mechanical valve integrity due
to abnormal connective tissue structure and function is the most common
finding.
Patients with fibroelastic deficiency are usually identified in their 60s.
Typically present with localized and unisegmental prolapse or flail
20.
Barlow’s Disease vs
Fiobroelastic
Deficiency
•Clear distinction between these
two entities is difficult because it
has been suggested that they
constitute the different ends of a
disease spectrum with some
valves not demonstrating the
typical appearance of Barlow
disease but having myxoid
infiltration on histopathological
exam.
21.
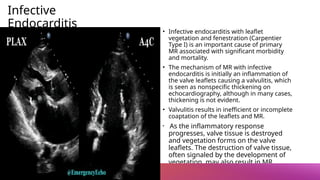
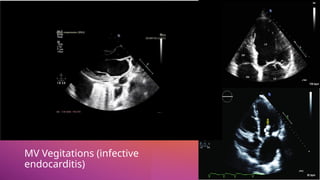
Infective
Endocarditis
• Infective endocarditiswith leaflet
vegetation and fenestration (Carpentier
Type I) is an important cause of primary
MR associated with significant morbidity
and mortality.
• The mechanism of MR with infective
endocarditis is initially an inflammation of
the valve leaflets causing a valvulitis, which
is seen as nonspecific thickening on
echocardiography, although in many cases,
thickening is not evident.
• Valvulitis results in inefficient or incomplete
coaptation of the leaflets and MR.
• As the inflammatory response
progresses, valve tissue is destroyed
and vegetation forms on the valve
leaflets. The destruction of valve tissue,
often signaled by the development of
vegetation, may also result in MR
Secondary Mitral Regurgitation
mainlya consequence of abnormal leaflet tethering forces due to LV or annular
distortion and dysfunction rather than valvular abnormalities (Carpentier Type IIIB).
The the mitral leaflets appear “normal” in secondary MR.
Altered LV geometry results in PM displacement, which in turn is associated with
increased leaflet tethering, resulting in the apical displacement of the coaptation zone
and incompetence of the MV
secondary MR is characterized by a significantly tented valve with restricted closure of
the valve leading to incomplete mitral leaflet closure
25.
Secondary Mitral
Regurgitation
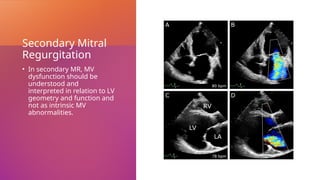
• Insecondary MR, MV
dysfunction should be
understood and
interpreted in relation to LV
geometry and function and
not as intrinsic MV
abnormalities.
26.
Secondary Mitral Regurgitation
Twodistinct entities of secondary MR can be defined according to the underlying
cause of the LV geometric alteration: ischemic and nonischemic MR.
Ischemic MR refers to mitral regurgitation that occurs as a result of left ventricular
remodeling and dysfunction due to coronary artery disease (CAD).
The most common mechanism of ischemic MR is characterized by increased MV
tethering as a consequence of acute or chronic regional or global LV
dilation/dysfunction and altered PM geometry.
According to the distribution of CAD and the location of the ischemic myocardium,
the resulting severity of MR can vary significantly, even a small ischemic portion of
the myocardium can lead to significant MR with preserved overall LV ejection
fraction,
27.
Secondary Mitral Regurgitation
Inthe case of nonischemic MR, the pathophysiology is similar with the exception of the root cause
of the LV abnormalities
remodeling of the LV causes displacement of the PM(s), which increases tethering and
malcoaptation of the leaflets).
In the nonischemic subset of patients with secondary MR, there is usually more homogeneous
dilation of the LV but fundamentally, the mechanism is similar to that when the ventricular
abnormalities are ischemic.
annular dilation alone without LV dilation or dysfunction can be the mechanistic cause of secondary
MR.
This typically occurs in the setting of atrial fibrillation with concomitant annular dilation and
dysfunction and can be associated with significant MR.
28.
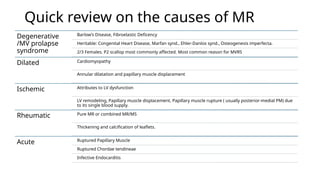
Quick review onthe causes of MR
Degenerative
/MV prolapse
syndrome
Barlow’s Disease, Fibroelastic Deficency
Heritable: Congenital Heart Disease, Marfan synd., Ehler-Danlos synd., Osteogenesis imperfecta.
2/3 Females. P2 scallop most commonly affected. Most common reason for MVRS
Dilated Cardiomyopathy
Annular dilatation and papillary muscle displacement
Ischemic Attributes to LV dysfunction
LV remodeling, Papillary muscle displacement, Papillary muscle rupture ( usually posterior-medial PM) due
to its single blood supply.
Rheumatic Pure MR or combined MR/MS
Thickening and calcification of leaflets.
Acute Ruptured Papillary Muscle
Ruptured Chordae tendineae
Infective Endocarditis
29.
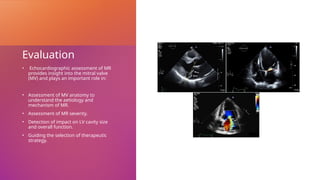
Evaluation
• Echocardiographic assessmentof MR
provides insight into the mitral valve
(MV) and plays an important role in:
• Assessment of MV anatomy to
understand the aetiology and
mechanism of MR.
• Assessment of MR severity.
• Detection of impact on LV cavity size
and overall function.
• Guiding the selection of therapeutic
strategy.
30.
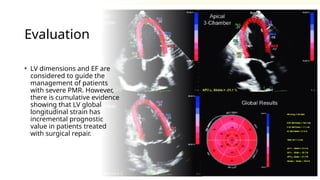
Evaluation
• LV dimensionsand EF are
considered to guide the
management of patients
with severe PMR. However,
there is cumulative evidence
showing that LV global
longitudinal strain has
incremental prognostic
value in patients treated
with surgical repair.
31.
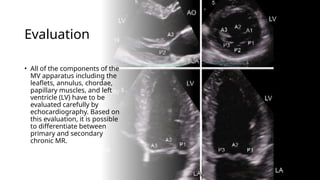
Evaluation
• All ofthe components of the
MV apparatus including the
leaflets, annulus, chordae,
papillary muscles, and left
ventricle (LV) have to be
evaluated carefully by
echocardiography. Based on
this evaluation, it is possible
to differentiate between
primary and secondary
chronic MR.
32.
Evaluation
In chronic primaryMR, echocardiography
helps in:
•Detailed assessment of the MV leaflets to
diagnose prolapsed scallop(s), flail leaflet,
perforation, vegetation, etc.
•Detailed assessment of the subvalvular
apparatus to diagnose ruptured chordae,
ruptured papillary muscle.
In chronic secondary MR, echocardiography
helps in:
•Volumetric measurement of LV size and
ejection fraction.
•Assessment of global and regional wall
motion abnormalities of the LV.
•Tethering of the MV leaflet due to papillary
muscle displacement.
•Symmetric or asymmetric mitral annulus
dilatation.
33.
Evaluation
• Many parameters(qualitative, semi-quantitative and
quantitative) can be used to define the severity of MR.
None of them can be relied on solely for the
definition. An integrative approach to include most of
them is a must to achieve accurate diagnosis and
overcome the pitfalls and limitations of each
parameter
34.
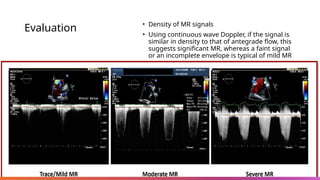
Evaluation • Densityof MR signals
• Using continuous wave Doppler, if the signal is
similar in density to that of antegrade flow, this
suggests significant MR, whereas a faint signal
or an incomplete envelope is typical of mild MR
35.
Evaluation
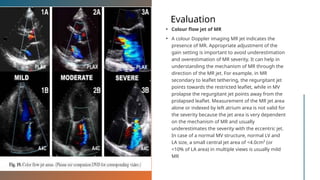
• Colour flowjet of MR
• A colour Doppler imaging MR jet indicates the
presence of MR. Appropriate adjustment of the
gain setting is important to avoid underestimation
and overestimation of MR severity. It can help in
understanding the mechanism of MR through the
direction of the MR jet. For example, in MR
secondary to leaflet tethering, the regurgitant jet
points towards the restricted leaflet, while in MV
prolapse the regurgitant jet points away from the
prolapsed leaflet. Measurement of the MR jet area
alone or indexed by left atrium area is not valid for
the severity because the jet area is very dependent
on the mechanism of MR and usually
underestimates the severity with the eccentric jet.
In case of a normal MV structure, normal LV and
LA size, a small central jet area of <4.0cm² (or
<10% of LA area) in multiple views is usually mild
MR
36.
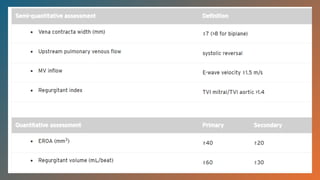
Evaluation: Semi-
quantitative
assessment
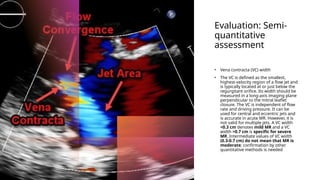
• Venacontracta (VC) width
• The VC is defined as the smallest,
highest-velocity region of a flow jet and
is typically located at or just below the
regurgitant orifice. Its width should be
measured in a long-axis imaging plane
perpendicular to the mitral leaflet
closure. The VC is independent of flow
rate and driving pressure. It can be
used for central and eccentric jets and
is accurate in acute MR. However, it is
not valid for multiple jets. A VC width
<0.3 cm denotes mild MR and a VC
width >0.7 cm is specific for severe
MR. Intermediate values of VC width
(0.3-0.7 cm) do not mean that MR is
moderate; confirmation by other
quantitative methods is needed
37.
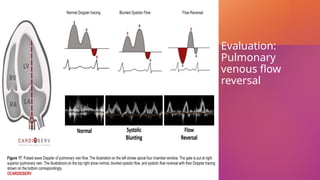
Evaluation: Pulmonary venousflow
reversal
• Reduced systolic velocity in >1 pulmonary
vein and even reverse flow indicates
severe MR. However, increased left atrial
pressure of any cause can result in
blunted pulmonary venous systolic flow
(Figure 1D). Absence of flow reversal
should not be used for exclusion of
significant MR. It can be false negative if
the jet is directed away from pulmonary
veins, e.g., highly eccentric MR and/or
severely dilated left atrium. On the other
hand, if the MR jet is small but eccentric
and directed towards the pulmonary
vein, blunted or reverse flow can be
recorded in this pulmonary vein (false
positive).
Evaluation: Peak
velocity ofE-wave
of MV inflow
• Using pulsed Doppler at the tip
of the MV, early filling (E-wave)
usually dominant (E velocity >1.5
m/s) indicates severe MR due to
increased forward flow across
the MV. If the A-wave is
dominant, severe MR can be
excluded
40.
Regurgitant index
• Anon-geometric pulsed Doppler index, namely the
mitral to aortic velocity-time integral (VTI), is used for
quantification of pure isolated organic MR. A ratio
1.4 defines patients with severe MR with a
≥
sensitivity of 87%, and a specificity of 91%.
41.
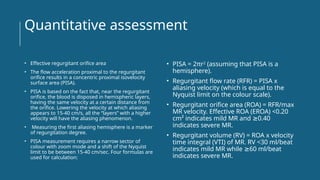
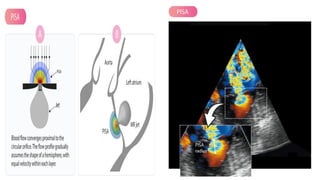
Quantitative assessment
• Effectiveregurgitant orifice area
• The flow acceleration proximal to the regurgitant
orifice results in a concentric proximal isovelocity
surface area (PISA).
• PISA is based on the fact that, near the regurgitant
orifice, the blood is disposed in hemispheric layers,
having the same velocity at a certain distance from
the orifice. Lowering the velocity at which aliasing
appears to 15-40 cm/s, all the “layers” with a higher
velocity will have the aliasing phenomenon.
• Measuring the first aliasing hemisphere is a marker
of regurgitation degree.
• PISA measurement requires a narrow sector of
colour with zoom mode and a shift of the Nyquist
limit to be between 15-40 cm/sec. Four formulas are
used for calculation:
• PISA = 2πr2
(assuming that PISA is a
hemisphere).
• Regurgitant flow rate (RFR) = PISA x
aliasing velocity (which is equal to the
Nyquist limit on the colour scale).
• Regurgitant orifice area (ROA) = RFR/max
MR velocity. Effective ROA (EROA) <0.20
cm² indicates mild MR and 0.40
≥
indicates severe MR.
• Regurgitant volume (RV) = ROA x velocity
time integral (VTI) of MR. RV <30 ml/beat
indicates mild MR while 60 ml/beat
≥
indicates severe MR.
Medical Therapy
in Primary
Mitral
regurgitation
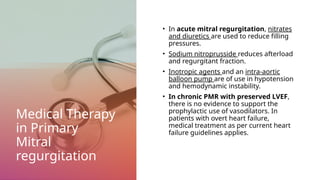
•In acute mitral regurgitation, nitrates
and diuretics are used to reduce filling
pressures.
• Sodium nitroprusside reduces afterload
and regurgitant fraction.
• Inotropic agents and an intra-aortic
balloon pump are of use in hypotension
and hemodynamic instability.
• In chronic PMR with preserved LVEF,
there is no evidence to support the
prophylactic use of vasodilators. In
patients with overt heart failure,
medical treatment as per current heart
failure guidelines applies.
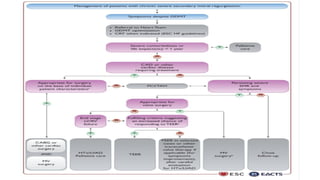
Medical therapy in
SecondaryMitral
regurgitation
• Optimal medical therapy, in line with the
guidelines for the management of heart
failure, should be the first and essential
step in the management of all patients
with SMR and should include replacement
of ACEI or ARB with Sacubitril/valsartan,
sodium-glucose cotransporter 2
inhibitors and/or ivabradine, whenever
indicated.
• Indications for cardiac resynchronization
therapy (CRT) should be evaluated in
accordance with related guidelines.
• If symptoms persist after optimization of
conventional heart failure therapy, options
for mitral valve intervention should be
promptly evaluated before further
deterioration of LV systolic function or
cardiac remodeling occur.
References
• Feigenbaum’s echocardiography/ William F. Armstrong,
Thomas Ryan. Eighth edition.
• Essential echocardiography : a companion to
Braunwald’s Heart disease 2019
• European Society of Cardiology : Valvular Heart Disease
Guidelines; Mitral Regurgitation.
• Pausch, J., Bhadra, O., Mersmann, J. et al. prognostic
impact of functional mitral regurgitation prior to left
ventricular assist device implantation. J cardiothorac Surg
17, 24 (2022). http://doi.org/10.1186/s13019-021-01748-9
• Anwar, A.M. (2018). Understanding the role of
echocardiography in the assessment of mitral valve dis.
[online] Escardio.org. Available at:
https://www.escardio.org/Journals/E-Journal-of-
Cardiology-Practice/Volume-16/Understanding-the-role-
of-echocardiography-in-the-assessment-of-mitral-valve-
disease [Accessed 9 Feb. 2024
• Abbott Vascular website : www.abbottvascular.com







![References
• Feigenbaum’s echocardiography / William F. Armstrong,
Thomas Ryan. Eighth edition.
• Essential echocardiography : a companion to
Braunwald’s Heart disease 2019
• European Society of Cardiology : Valvular Heart Disease
Guidelines; Mitral Regurgitation.
• Pausch, J., Bhadra, O., Mersmann, J. et al. prognostic
impact of functional mitral regurgitation prior to left
ventricular assist device implantation. J cardiothorac Surg
17, 24 (2022). http://doi.org/10.1186/s13019-021-01748-9
• Anwar, A.M. (2018). Understanding the role of
echocardiography in the assessment of mitral valve dis.
[online] Escardio.org. Available at:
https://www.escardio.org/Journals/E-Journal-of-
Cardiology-Practice/Volume-16/Understanding-the-role-
of-echocardiography-in-the-assessment-of-mitral-valve-
disease [Accessed 9 Feb. 2024
• Abbott Vascular website : www.abbottvascular.com](https://image.slidesharecdn.com/mitralregurgitationibrahimghazi-250424190948-8729187a/85/Mitral-Regurgitation-evaluationofprostheticvalvefunctio-53-320.jpg)
















































