Anaerobic Infections
Dr. MohamedSakr, M.D.
Medical Microbiology and Immunology
Start
Think
Analysis
Planning
Try
Do
Do again
Keep On
Doing
Success
2.
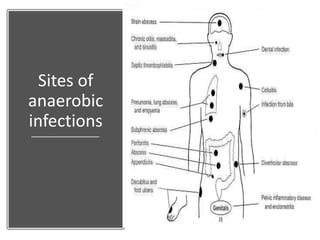
Sources of AnaerobicInfections
• Endogenous (from body)
– Intestinal anaerobes
– Oral anaerobes
– Skin glands and hair follicles
• Exogenous (Soil)
– Clostridium tetani (tetanus)
– Clostridium botulinum (botulism)
– Clostridium difficile (antibiotic-associated colitis)
• Either endogenous or exogenous
An anaerobic organism is any organism
that does not require oxygen for growth.
3.
Categories of anaerobes:
Obligateanaerobes, which are harmed by
the presence of oxygen.
Aerotolerant organisms, which cannot use
oxygen for growth, but tolerate its presence.
Microaerophilic bacteria need oxygen because they
cannot ferment or respire anaerobically. However,
they are poisoned by high concentrations of
oxygen.
Facultative anaerobes, which can grow
without oxygen but use oxygen if it is
present.
4.
Obligate
anaerobes
• These bacteriacannot grow in
the presence of oxygen
• Furthermore, they are killed
by oxygen; they lack enzymes
such as catalase, peroxidase
and superoxide dismutase.
These enzymes detoxify
oxygen toxic products results
from aerobic metabolic
reactions.
• Anaerobic bacteria use
glycolysis and fermentation
to gain energy.
5.
Do you think
thatAnaerobes
have a role in
normal host
physiology?
– Prevent colonization &
infection by pathogens
• Bacterial interference
through elaboration of
toxic metabolites, low
pH, depletion of
nutrients
• Interference with
adhesion
– Contributes to host
physiology
• B. fragilis synthesizes
vitamin K and
deconjugates bile acids
Bacteriological finding suggestiveof
anaerobic infection
• Typical morphology for anaerobes on Gram stain
• Inability to grow in aerobic cultures
• Anaerobic growth on proper media containing
antibiotic-suppressing aerobes
• Growth in anaerobic zone of fluid or agar media
• Growth anaerobically on media containing
Kanamycin, neomycin or vancomycin.
8.
Bacteriological finding suggestiveof
anaerobic infection
• Gas, foul-smelling odour in specimen or
bacterial culture
• Young colonies of pigmented Prevotella and
Porphyromonas may fluoresce red under
ultraviolet light, and older colonies produce a
typical dark pigment
• Characteristic colonies on agar plates under
anaerobic conditions (e.g. Clostridium
perfringens, Fusobacterium nucleatum).
Anaerobic gram positivebacilli
• No Spore Formation
– Propionibacterium
• P. acnes
– Actinomyces
• A. israelii
– Lactobacillus
– Mobiluncus
• Spore Formation
– Clostridium
• C.
perfringens
• C. difficile
• C. tetani
• C. botulinum
12.
Clostridia
• Large, Gram-positive,anaerobic bacilli - All species form
endospores and most of them are saprophytes.
• Live in the anaerobic habitats of nature, including soils and the
intestinal tracts of animals.
Clinically important species
• Clostridium tetani causing tetanus.
• Clostridium perfringens causing gas gangrene.
• C. difficile causing pseudomembranous colitis.
• Clostridium botulinum (food-borne botulism in inadequately sterilized
canned food) produce very potent biological toxins that affect humans.
14.
Clostridium tetani
• Gram-positivebacilli that forms a terminal
spore
• Common resident of soil and GI tracts of
animals and humans.
• Causes tetanus or lockjaw, a neuromuscular
serious bacterial disease that affects your
nervous system, leading to painful muscle
contractions, particularly of your jaw and neck
muscles.
• Most commonly among geriatric patients and IV
drug abusers; neonates in developing countries
15.
Pathogenicity and wayof infection
• Spores usually enter through accidental puncture wounds,
burns, umbilical stumps, frostbite, and crushed body
parts.
• Anaerobic environment is ideal for vegetative cells to
grow and release tetanospasmin and tetanolysin toxins.
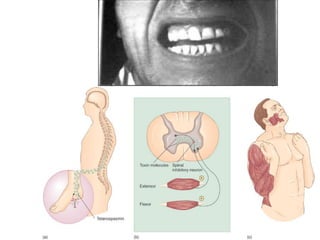
• Tetanospasmin is neurotoxin causes paralysis by binding
to motor nerve endings; blocking the release of inhibitory
mediators required for muscular contraction inhibition
leading to uncontralable painful muscle contractions.
• It is transported within the axon and across synaptic
junctions until it reaches the central nervous system.
Because inhibitory neurons are involved, the result is
unopposed muscle contraction.
16.
The common signsand symptoms
• The common signs and symptoms of tetanus
include:
➢Spasms and stiffness in jaw muscles (trismus)
➢Stiffness of neck muscles
➢Difficulty swallowing
➢Stiffness of your abdominal muscles
➢Painful body spasms lasting for several minutes
• Death most often due to paralysis of respiratory
muscles (Unlikely in this case)
18.
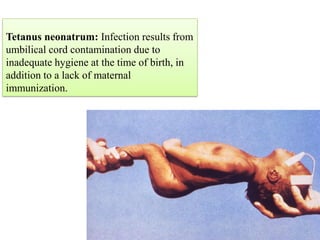
Tetanus neonatrum: Infectionresults from
umbilical cord contamination due to
inadequate hygiene at the time of birth, in
addition to a lack of maternal
immunization.
19.
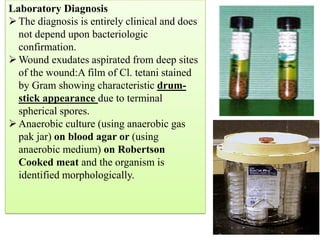
Laboratory Diagnosis
➢The diagnosisis entirely clinical and does
not depend upon bacteriologic
confirmation.
➢Wound exudates aspirated from deep sites
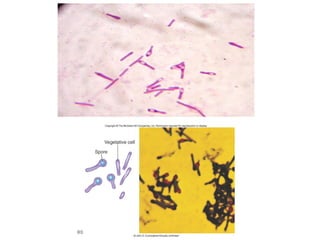
of the wound:A film of Cl. tetani stained
by Gram showing characteristic drum-
stick appearance due to terminal
spherical spores.
➢Anaerobic culture (using anaerobic gas
pak jar) on blood agar or (using
anaerobic medium) on Robertson
Cooked meat and the organism is
identified morphologically.
The meat's function is to absorb the oxygen from the fluid
by releasing reducing agents.
20.
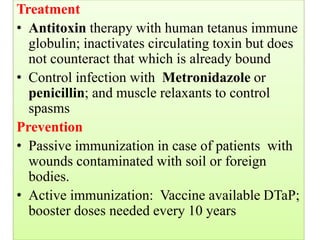
Treatment
• Antitoxin therapywith human tetanus immune
globulin; inactivates circulating toxin but does
not counteract that which is already bound
• Control infection with Metronidazole or
penicillin; and muscle relaxants to control
spasms
Prevention
• Passive immunization in case of patients with
wounds contaminated with soil or foreign
bodies.
• Active immunization: Vaccine available DTaP;
booster doses needed every 10 years
for neutralization early before it reaches the motor plate
before infection
after infection + needs antitoxin because it doesn't have a role in
the infection its only used for future exposure
D – Diphtheria
T – Tetanus
aP – acellular Pertussis
''The Triple Vaccine''
21.
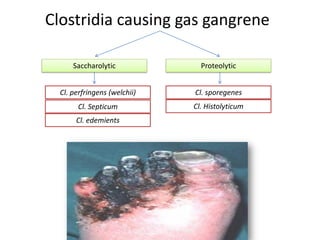
Clostridia causing gasgangrene
Saccharolytic Proteolytic
Cl. perfringens (welchii) Cl. sporegenes
Cl. Septicum Cl. Histolyticum
Cl. edemients
Breaks down
carbohydrates (use sugar
in the culture media)
Breaks down protein (use ptn
content in the culture media)
most common
and most
important
22.
• Gas gangrene(myonecrosis) is caused by exotoxin-
producing Clostridium species,
• Clostridium perfringens most frequent clostridia
involved in soft tissue and wound infections which
is capsulated & nonmotile and spores are oval or
subterminal.
• Spores found in soil, intestine of humans and
animals.
• Predisposing factors: accidents, surgical incisions,
compound fractures, diabetic ulcers, puncture
wounds and gunshot wounds. how? imbalanced blood sugar level > Less
sensation in peripheral areas > Less blood supply >
Ulcer > Gas gangrene
23.
• Virulence factors
–Toxins:
•Alpha toxin is lecithinase produced by most clostridia
and has phospholipase C activity. This potent toxin
causes lysis of red blood cells, myocytes, fibroblasts,
platelets, and leukocytes.
• Enterotoxin: causing food poisoning
• Theta toxin: hemolysin and is toxic for heart
muscles
–Hyaluronidase
–DNase
–Collagenase
(breaks down lecithin)
(fatal)
breaks down hyaluronidase
breaks down DNA
breaks down collagen
24.
Pathogenesis
• Myonecrosis isa condition of necrotic damage, specific to
muscle tissue requires sever trauma as in accidents and
anaerobic conditions.
• These conditions stimulate spore germination, vegetative
growth and release of exotoxins, and other virulence factors.
• The saccharolytic group: Fermentation of muscle
carbohydrates results in the formation of gas and acid. The
gas separates the muscle fibres from its sheeth→cutting of
its blood supply → necrosis of tissue.
• The proteolytic group: proteolysis of necrotic muscle fibers
→Blackening and foul smell of the gangrenous tissue.
(associated with the break down of protein)
25.
Laboratory Diagnosis
➢The diagnosisis entirely clinical and does not
depend upon bacteriologic confirmation.
➢Wound exudates aspirated from deep sites of the
wound and stained by Gram: Large gram positive
capsulated bacilli, spores are oval or sub
terminal.
➢Anaerobic culture (using anaerobic gas pak jar)on
blood agar (complete hemolysis:
➢(using anaerobic medium) on Robertson Cooked
meat : Blackening of the meat with the production
of H2S.
(because it takes too long)
tetani : spores are terminal (at the end).
(due to the breakdown of protein)
(indicator that the clostridium is proteolytic)
26.
Laboratory Diagnosis
➢Biochemical reactions:Litmus milk is acidified
and shows stormy clot formation. Sugars are
fermented with acid and excessive gas production.
➢Animal pathogenicity: Spreading gangrenous
inflammation
➢ELISA assays for detection of major toxins.
When the bacteria is cultured on litmus milk it breaks down the
lactose producing acid which will turn the litmus red
(injecting the microorganism into the animal)
27.
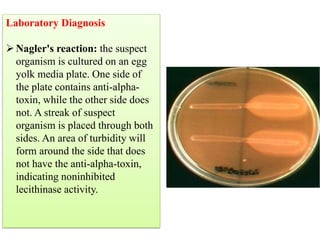
Laboratory Diagnosis
➢Nagler's reaction:the suspect
organism is cultured on an egg
yolk media plate. One side of
the plate contains anti-alpha-
toxin, while the other side does
not. A streak of suspect
organism is placed through both
sides. An area of turbidity will
form around the side that does
not have the anti-alpha-toxin,
indicating noninhibited
lecithinase activity.
explanation:
Microorganism is cultured on lecithin and divided into two
halves one has the antitoxin and the other doesn't
the half that has the antitoxin will be negative because the
antitoxin will neutralize the toxin and no reaction will occur.
the other half will appear cloudy which indicates that the
microorganism produced lecithinase and broke down the
lecithin.
28.
Treatment and Prevention
•Immediate cleansing of dirty wounds, decubitus
ulcers, compound fractures, and infected incisions.
• Debridement of disease tissue or even amputation
• Polyvalent antitoxic serum may be used.
• Large doses of cephalosporin or penicillin
• Hyperbaric oxygen therapy
• Fluid and electrolyte replacement
(removal of dead cells)
(no vaccine/immunization)
29.
Clostridial food poisoning
•Clostridium perfringens and its toxins are
found everywhere in the environment, and
human infection is most likely to come from
eating food with Clostridium perfringens in it
• Associated with undercooked meats or
reheated meat dishes.
• Most outbreaks come from food whose
temperature is poorly controlled. If food is
kept between 20 and 50 °C, it is likely to grow
Clostridium perfringens bacteria.
30.
Diagnosis & Managementof Clostridial
Food Poisoning
• People generally experience symptoms of Clostridium
perfringens infection 6 to 24 hours after consuming the
bacteria or toxins.
• Clostridium perfringens toxins cause abdominal pain and
stomach cramps, followed by diarrhea. Nausea is also a
common symptom.
• Illness from Clostridium perferingens generally lasts around
24 hours, and is rarely fatal.
• Treatment is symptomatic only as it is self limiting disease.
31.
Clostridium botulinum
• Gram-positivebacilli, anaerobic, oval or
subterminal spore-forming, motile bacterium
with the ability to produce the neurotoxin
botulinum.
• Commonly isolated in soil and water
• Human botulism associated with A, B, E & F
types
32.
Clostridium botulinum
Pathogenesis
Pre-formed exotoxinfrom prior germination of
spores may be present in inadequately autoclaved
canned food (usually at home).
Lethal dose for man is about 1-2 microgram.
• The toxin binds to receptors on peripheral nerves,
where acetylcholine is the neurotransmitter and
inhibits nerve impulses.
• Flaccid paralysis and often death from respiratory
and/or cardiac failure.
• The toxin is heat labile and can be destroyed if
heated at 100°C for 20 minutes.
33.
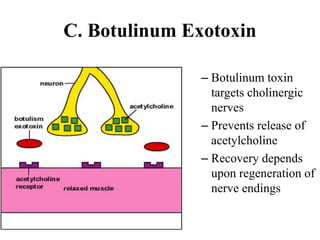
C. Botulinum Exotoxin
–Botulinum toxin
targets cholinergic
nerves
– Prevents release of
acetylcholine
– Recovery depends
upon regeneration of
nerve endings
34.
Botulism
• Clinical features(No GIT manifestations)
– Classical Foodborne botulism
• Mostly associated with home-canned foods and
preformed toxin
• After an incubation period of 72 hrs: blurred vision,
dilated pupils, dry mouth, difficulty in speech and
dysphagia
• Bilateral descending weakness of peripheral muscles;
death related to respiratory failure and/or cardiac failure
– Infant botulism
• Consumption of foods contaminated with botulinum
spores
• Disease associated with neurotoxin produced in vivo
– Wound botulism: rare
35.
Diagnosis of Botulism
Basedmainly on clinical diagnosis and
treatment should not wait for the lab
confirmation
–Isolation of toxin in food remnants or patient
blood
• PCR, Mouse bioassay & ELISA.
–Isolation of organism
• Culture implicated food and stool of
patient or gastric contents by gastric
lavage.
36.
Treatment & Preventionof Botulism
• Treatment
– Trivalent botulinum antitoxin (A, B, E) to bind
circulating botulinum toxin
– Supportive care
– Elimination of organism from GI tract
• Gastric lavage
• Metronidazole or penicillin
• Prevention
– Prevention of spore germination (Acid PH, storage
<4°C)
– Destruction of preformed toxin (20 min at 100°C)
37.
Clostridium difficile
Mode ofinfection:
Endogenous infection
• antibiotic exposure associated with overgrowth of
C. difficile
Exogenous infection
• spores detected in hospital rooms of infected
patients
• Risk factors:
➢ prolonged use of antibiotics
➢ Old age
➢ undergone gastrointestinal surgery, or
➢ have a serious underlying illness, or who are
immunocompromised.
38.
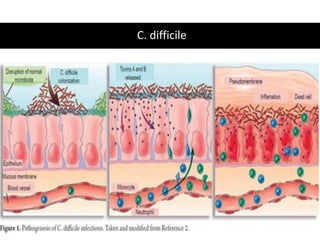
Clostridium difficile
• Pathogenesis
•Overgrowth of Clostridium difficile with
production of toxins in the colon
• Usually after the normal intestinal microbiota
flora has been disturbed by antimicrobial
chemotherapy especially clinadamycin and
cephlosporins.
C. difficile toxins:
• Toxin A is referred to as an enterotoxin because it
causes fluid accumulation in the bowel.
• Toxin B is an extremely lethal (cytopathic) toxin.
C. difficile
• Clinicalfeatures
– Asymptomatic colonization
– Fever, abdominal pain & diarrhea
– Pseudomembranous colitis
• Diagnosis
– Isolation of cytotoxin or enterotoxin in stools
• Treatment
– Discontinue antibiotics
– Metronidazole or vancomycin
– Supportive therapy: (fluid replacement, Toxin adsorbents &
Probiotics).
41.
Propionobacterium
• Produces propionicacid as major byproduct of
fermentation
• Commonly isolated from the flora of the face, chest,
and axilla region & female GU tract
• P. acnes
• a major pathogen responsible for postoperative shoulder infections
after both arthroscopy and arthroplasty procedures.
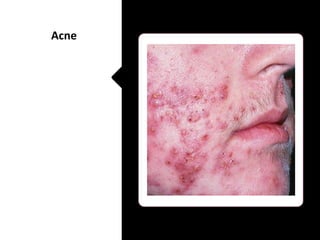
Acne
• Resides in sebaceous follicles, releases LMW peptide, stimulates an
inflammatory response
Opportunistic infections
• Prosthetic devices (heart valves, CSF shunts)
Actinomyces
Actinomyces israelii isthe most prevalent species
isolated in human infections.
• Facultative or strict anaerobes
• normally colonize the human mouth and digestive
and genital tracts.
• Development of disease when normal mucosal
barriers are disrupted
Clinical forms of actinomycosis are cervicofacial,
thoracic, and abdominal.
44.
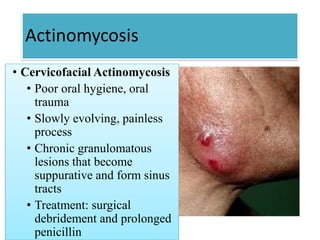
Actinomycosis
• Cervicofacial Actinomycosis
•Poor oral hygiene, oral
trauma
• Slowly evolving, painless
process
• Chronic granulomatous
lesions that become
suppurative and form sinus
tracts
• Treatment: surgical
debridement and prolonged
penicillin
45.
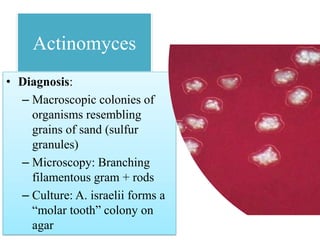
Actinomyces
• Diagnosis:
– Macroscopiccolonies of
organisms resembling
grains of sand (sulfur
granules)
– Microscopy: Branching
filamentous gram + rods
– Culture: A. israelii forms a
“molar tooth” colony on
agar
46.
Lactobacillus
• Facultative orstrict anaerobes
• Colonize GI and GU tract
– Produces H2O2 which is bactericidal to Gardnerella
vaginalis
– Vagina heavily colonized by Lactobacillus crispatus &
jensenii
• Clinical features
– Transient bacteremia from GU source
– Endocarditis
– Bacteremia in immunocompromised host
47.
Mobiluncus
• Obligate anaerobes
•Colonize GU tract in low numbers
• Associated with bacterial vaginosis
– Detected in vagina of 6% of controls
48.
Anaerobic gram negativebacilli
• Bacteroides
– B. fragilis
• Fusobacterium
• Prevotella: part of normal flora of the upper
respiratory tract and female genital tract
• Porphyromonas: part of normal oral flora,
can be cultured from gingival and periapical
tooth infections.
Bacteroides
–B. fragilis associatedwith 80% of intra-
abdominal infection
• Pathogenesis
–Polysaccharide capsule
• Increases adhesion to peritoneal surfaces
(along with fimbriae)
• Antiphagocytic activity
–Elaborate a variety of enzymes
51.
Bacteroides
• Clinical features
–Intra-abdominal infections (peritonitis, abscess);
– Post-operative infection after bowel surgery
– Bacteremia
– Skin & soft tissue infections and diabetic ulcers
• Treatment
– Drainage of abscess and debridement of necrotic
tissue
– Antibiotics
52.
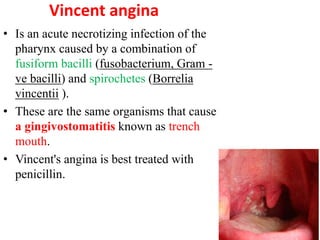
Vincent angina
• Isan acute necrotizing infection of the
pharynx caused by a combination of
fusiform bacilli (fusobacterium, Gram -
ve bacilli) and spirochetes (Borrelia
vincentii ).
• These are the same organisms that cause
a gingivostomatitis known as trench
mouth.
• Vincent's angina is best treated with
penicillin.
53.
Anaerobic cocci
–Part ofnormal flora of skin, mouth,
intestinal and genitourinary tracts
• Pathogenesis
–Opportunistic pathogens, often involved in
polymicrobial infections
–Brain abscesses, periodontal disease,
pneumonias, skin and soft tissue infections,
intra-abdominal infections
54.
Anaerobic cocci
• Peptostreptococcus (Gram positive cocci)
–P. magnus: chronic bone and joint
infections, especially prosthetic joints
–P. prevotii and P. anaerobius: female genital
tract and intra-abdominal infections
• Veillonella (Gram negative cocci)
–Normal oral flora; isolated from infected
human bites


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



