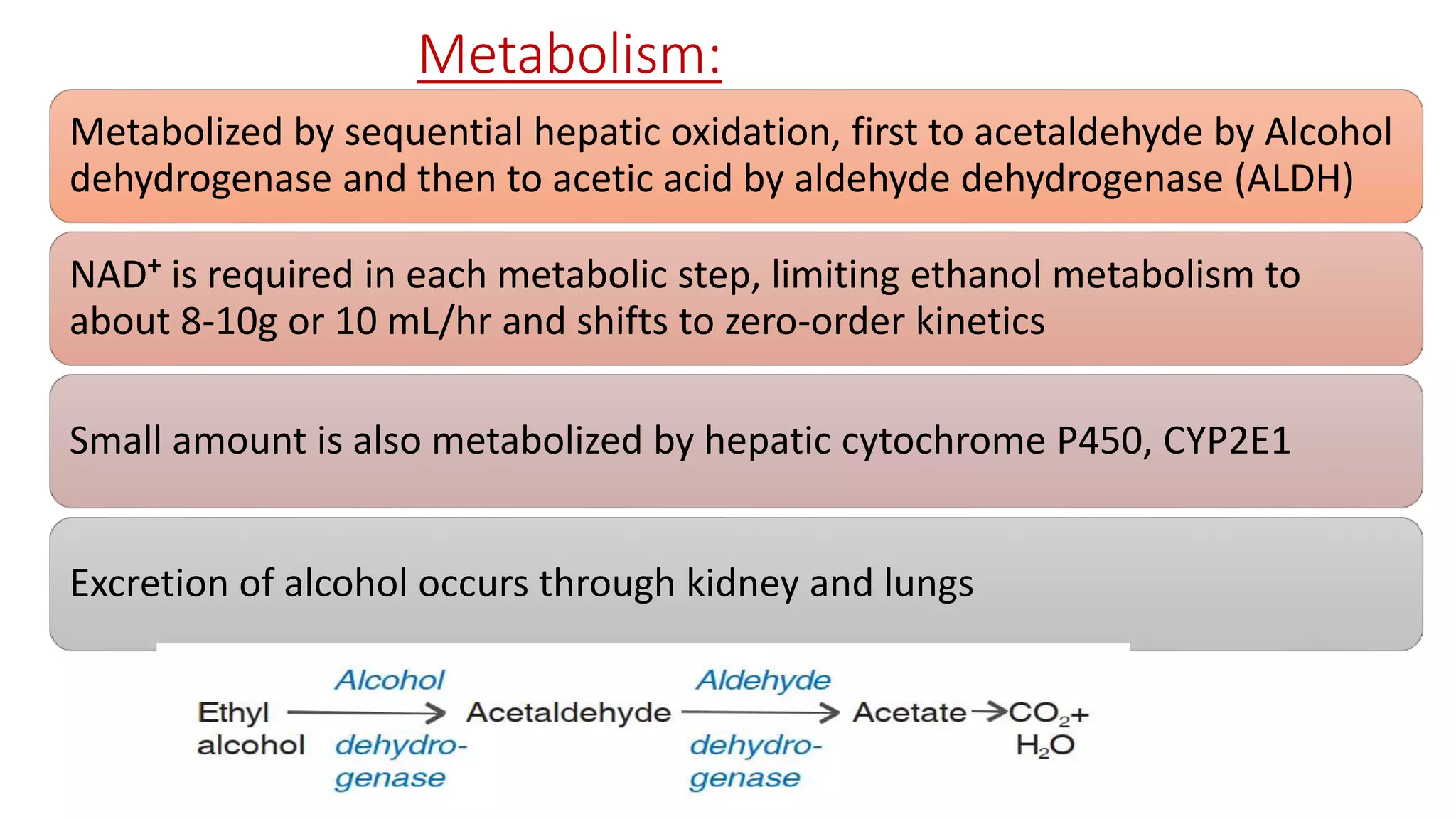
1) Ethanol is produced commercially by fermenting sugars or starches with yeast. It is then distilled to produce spirits with 40-55% alcohol content.
2) Acute ethanol intoxication causes symptoms like slurred speech and impaired coordination above 80mg/dL blood alcohol content. Treatment focuses on airway protection and supportive care.
3) Chronic heavy ethanol use can lead to tolerance, dependence, and withdrawal symptoms like tremors or seizures upon cessation. Approved medications like naltrexone and acamprosate aim to reduce craving and ease withdrawal.