Downloaded 89 times






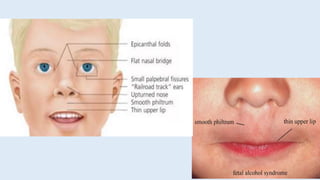




This document discusses alcohol poisoning and the effects of ethanol. It covers the categories of alcohols, ethanol uses including as a beverage and in medicine, toxicokinetics of ethanol absorption and metabolism, mechanisms of action on the body, acute and chronic poisoning symptoms, and treatment approaches for alcohol poisoning and chronic alcoholism.


































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)