The document provides an in-depth overview of aliphatic alcohols, focusing on the properties, pharmacological actions, and effects of ethanol and methanol, including their uses and toxicities. It discusses various aspects of alcohol consumption, including social implications, guidelines for moderate alcohol use, and the consequences of acute and chronic alcoholism. Additionally, it covers treatment options for alcohol dependence and methanol poisoning, along with preventive measures and pharmacological interventions.

![Toxicity
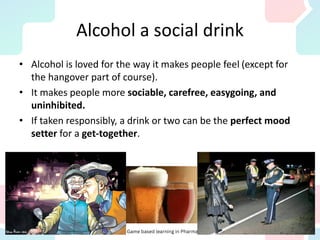
S/E of moderate drinking
Nausea, vomiting
Flushing, hangover, traffic accidents
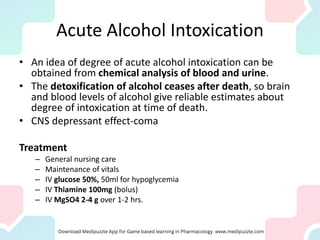
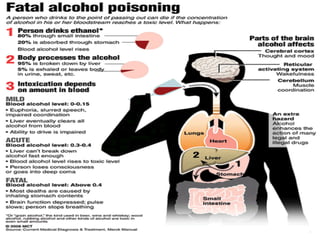
Acute alcohol intoxication
Hypotension, Hypoglycaemia, Gastritis
Collapse, Respiratory depression, Coma, Death
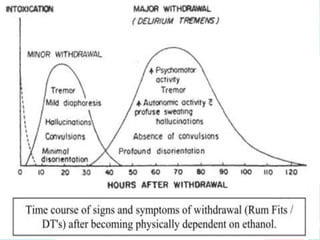
Chronic Alcoholism
Tolerance to subjective & behavioral effects
[reduced rate of absorption d/t gastritis, enzyme induction]
Psychic dependence with moderate drinking](https://image.slidesharecdn.com/x25e7h7tru322vwh9pzd-cns-alcohols-230313003533-29b432ac/85/CNS-_Alcohols-pdf-22-320.jpg)
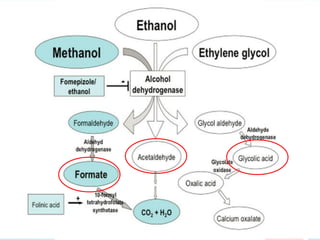
![Methanol poisoning
Methanol is the most toxic of the aliphatic alcohols.
Its oxidation leads to formaldehyde and formic acid.
Typical symptoms of methanol poisoning are visual
disorders (e.g., the impression of a snowstorm), which
can lead to blindness and even death.
[Loss of sight news from Nepal & Pakistan]
In the case of serious poisoning, one can actually smell
formaldehyde on the subject’s exhaled breath.](https://image.slidesharecdn.com/x25e7h7tru322vwh9pzd-cns-alcohols-230313003533-29b432ac/85/CNS-_Alcohols-pdf-47-320.jpg)