Downloaded 15 times
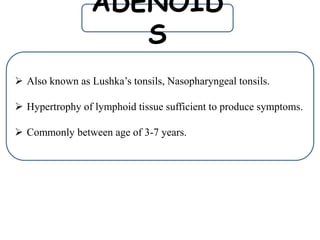


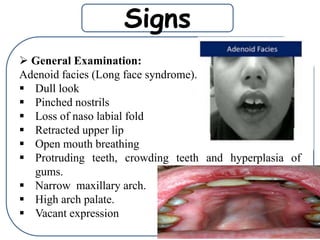









The document discusses adenoid hypertrophy, which commonly occurs in children ages 3-7. It causes nasal obstruction and symptoms like mouth breathing, snoring, ear infections, and speech problems. Examination findings include adenoid facies and nasal discharge. Diagnosis involves endoscopy to grade the adenoid size. Treatment is typically adenoidectomy to remove the enlarged adenoids.























































































