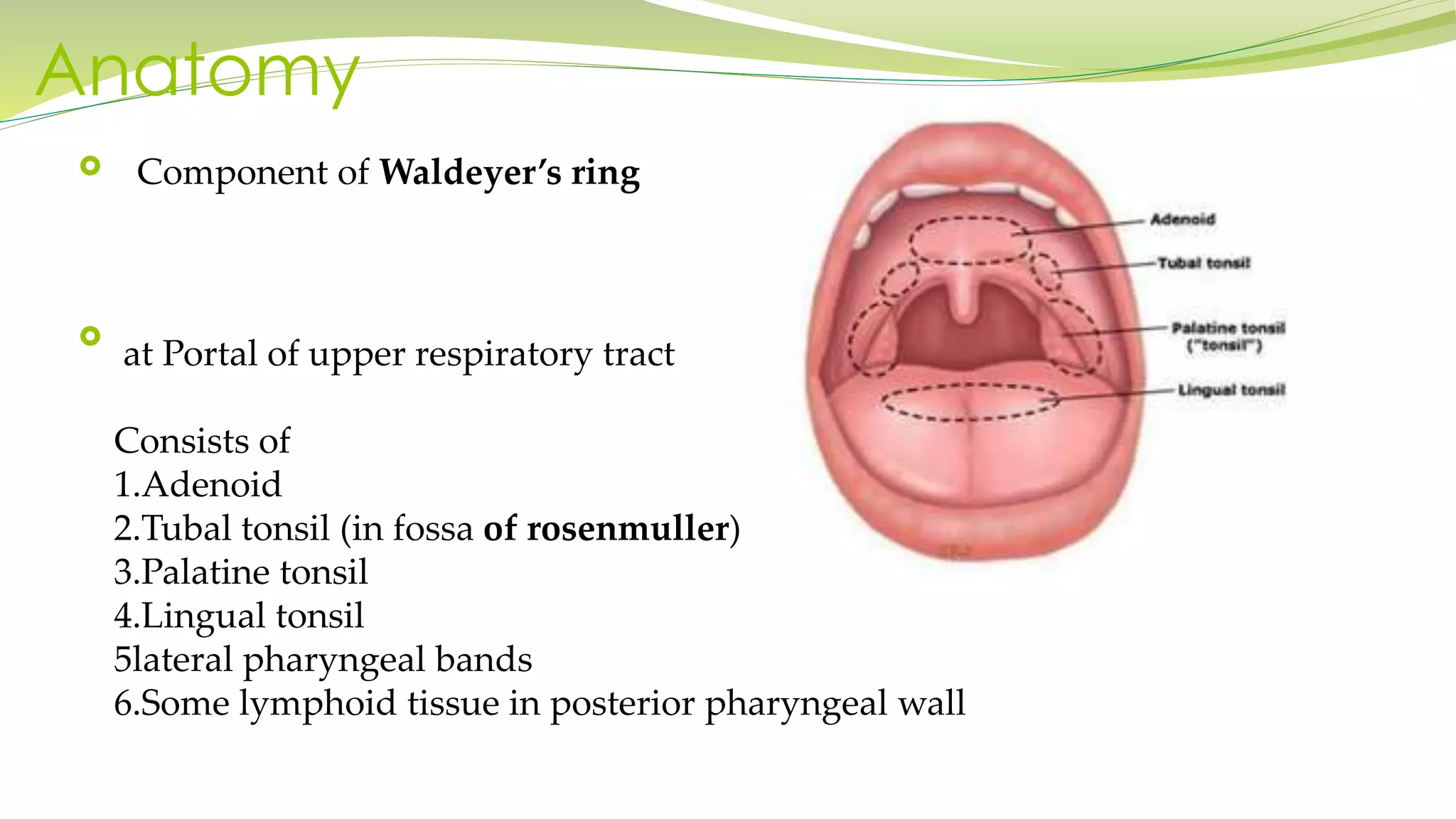
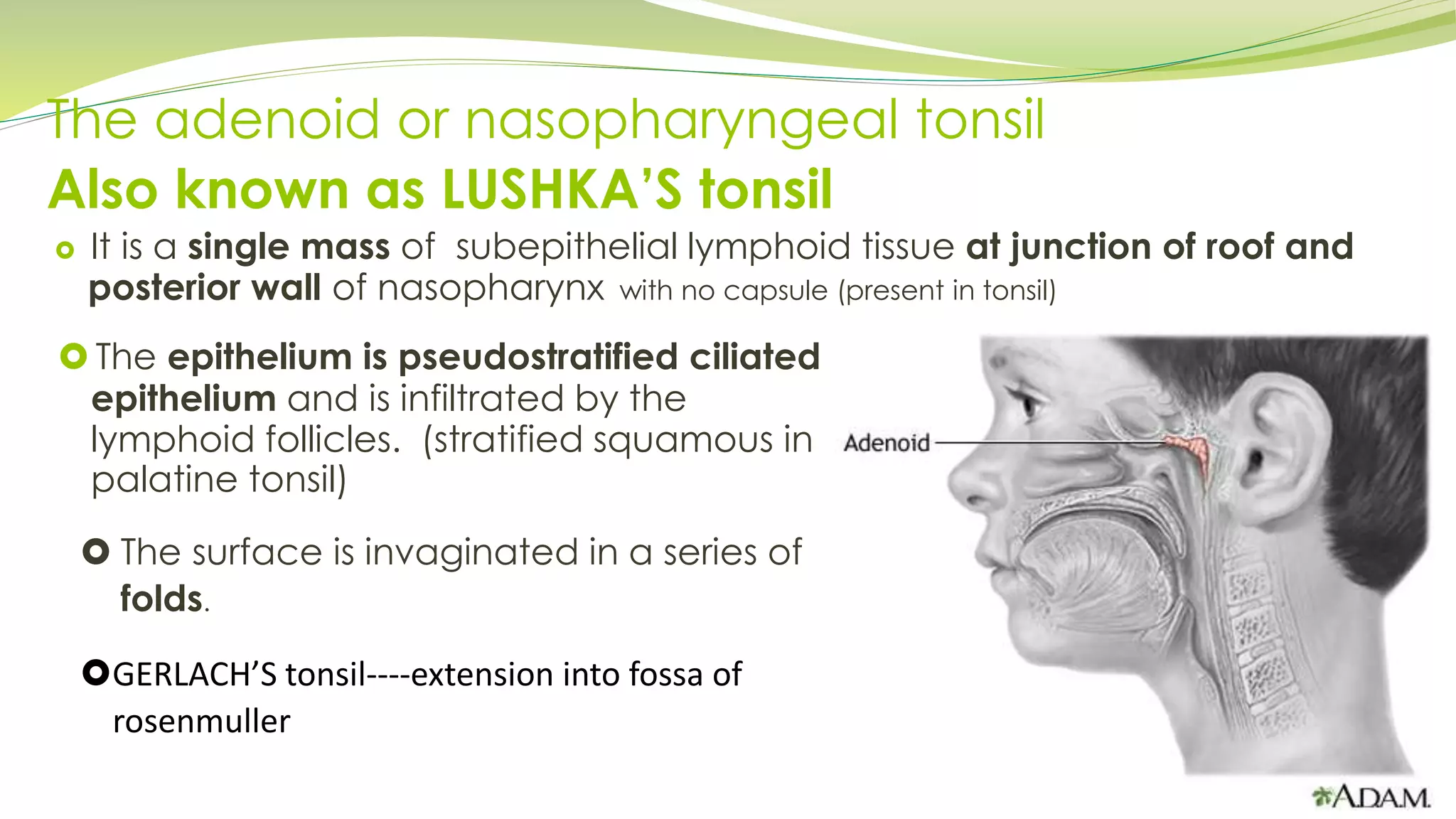
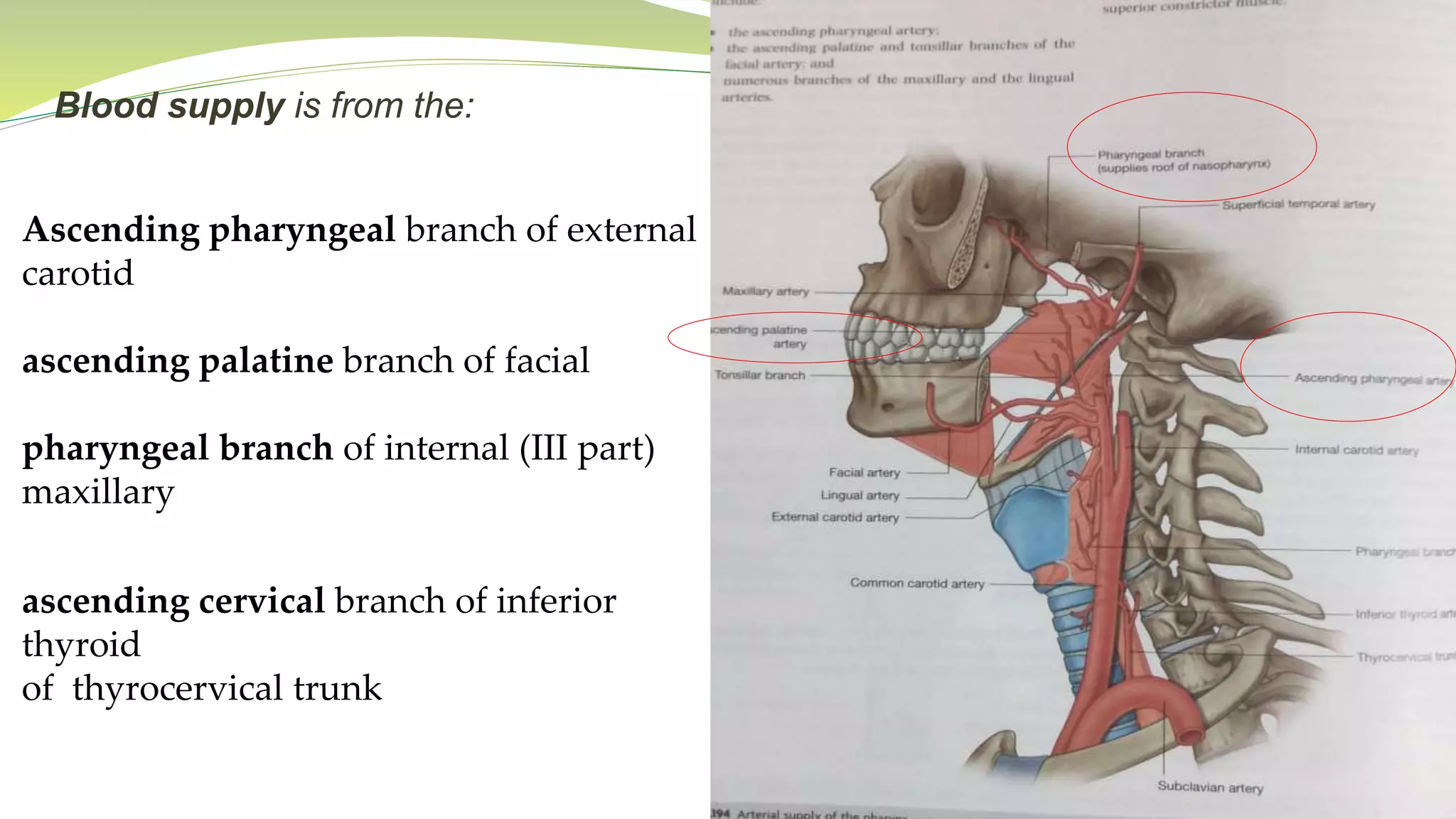
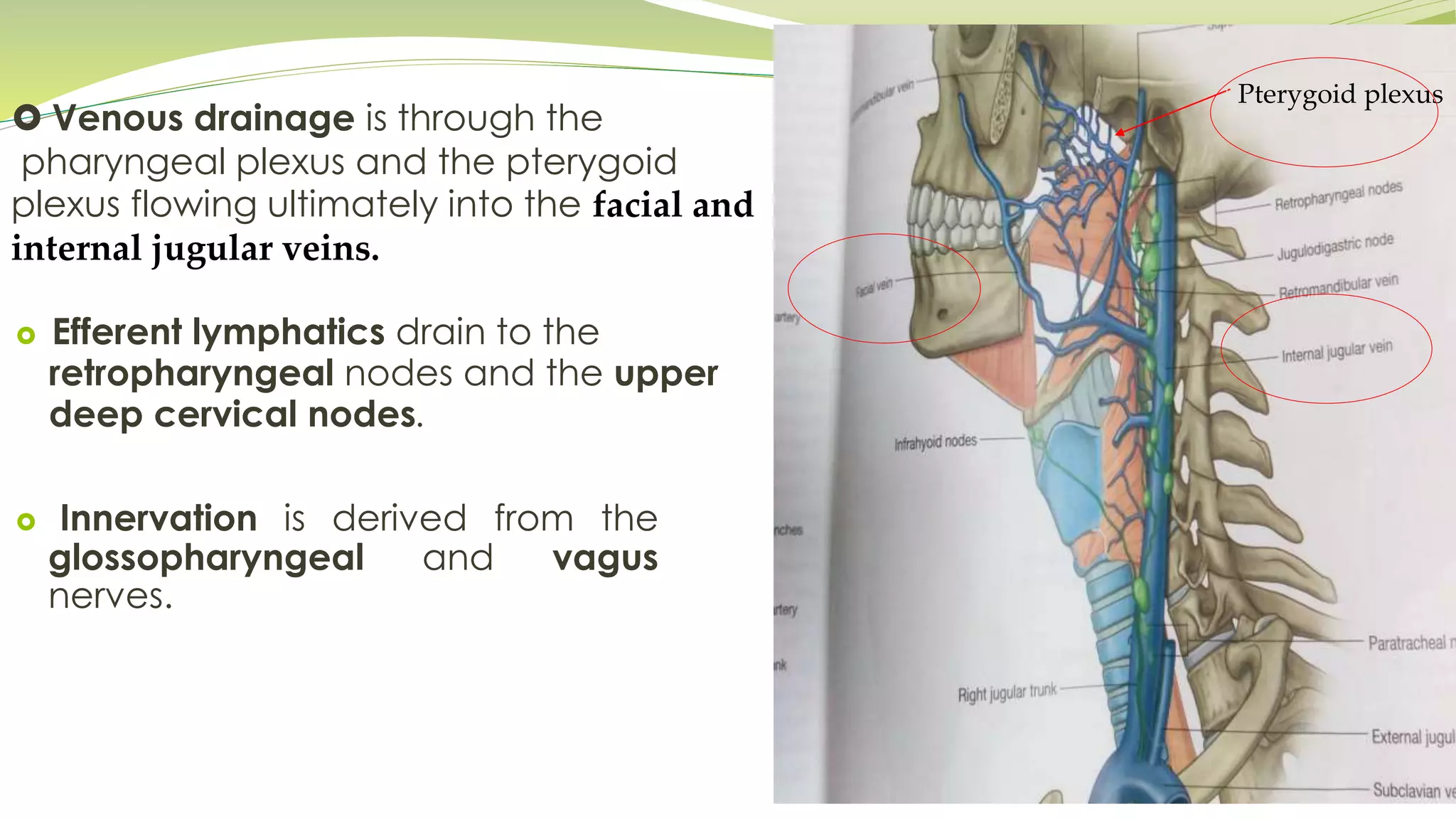
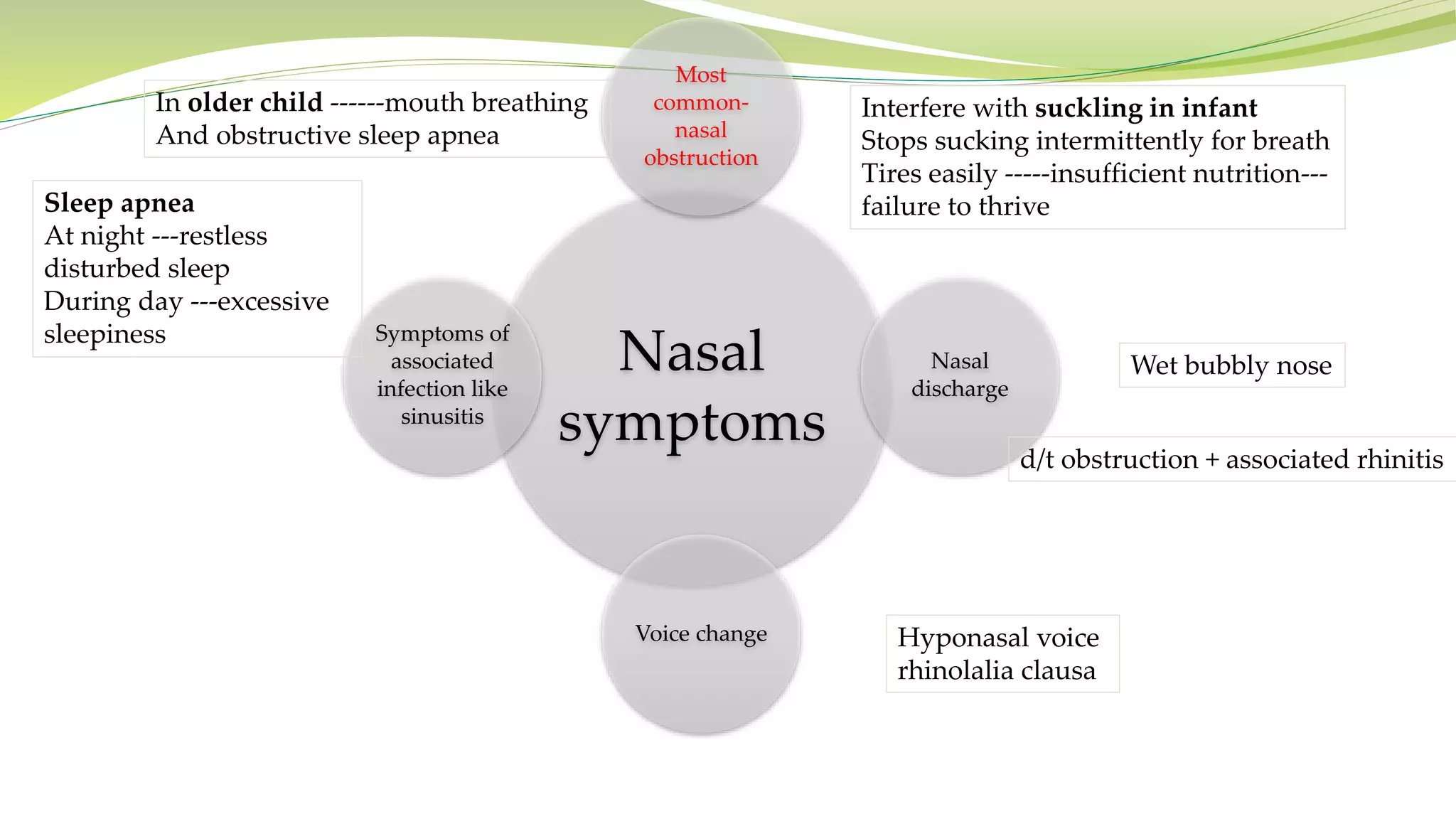
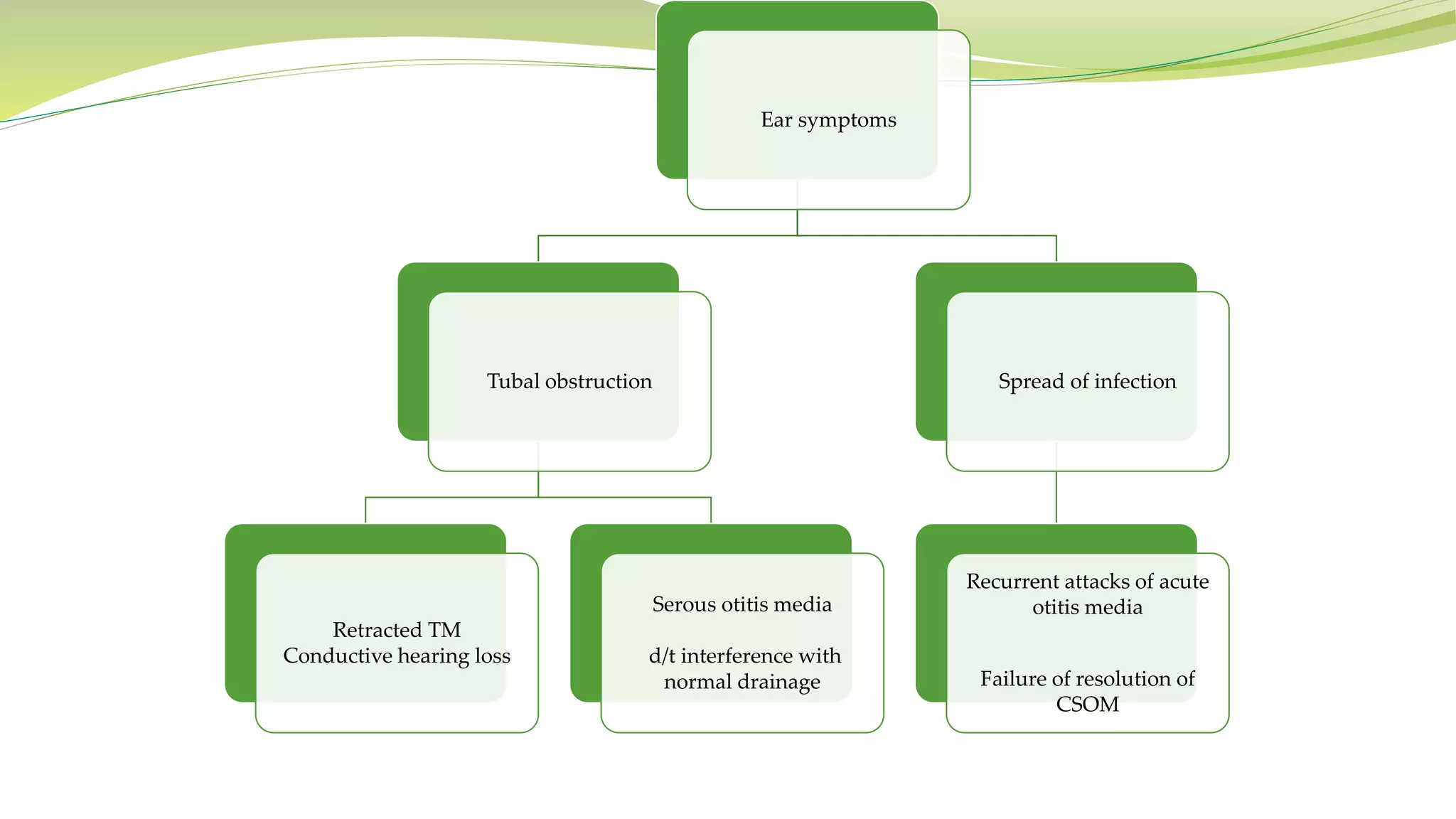
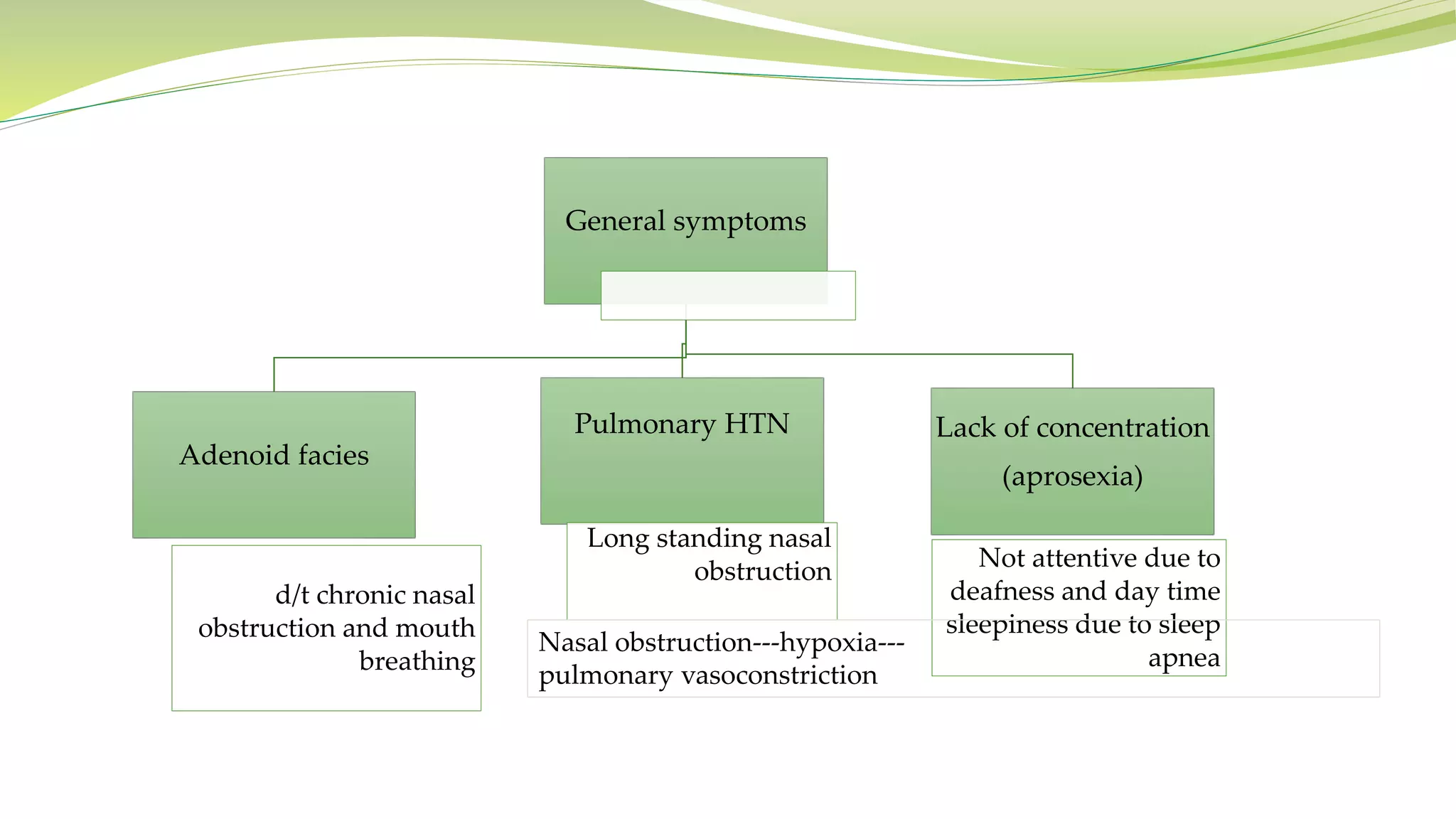
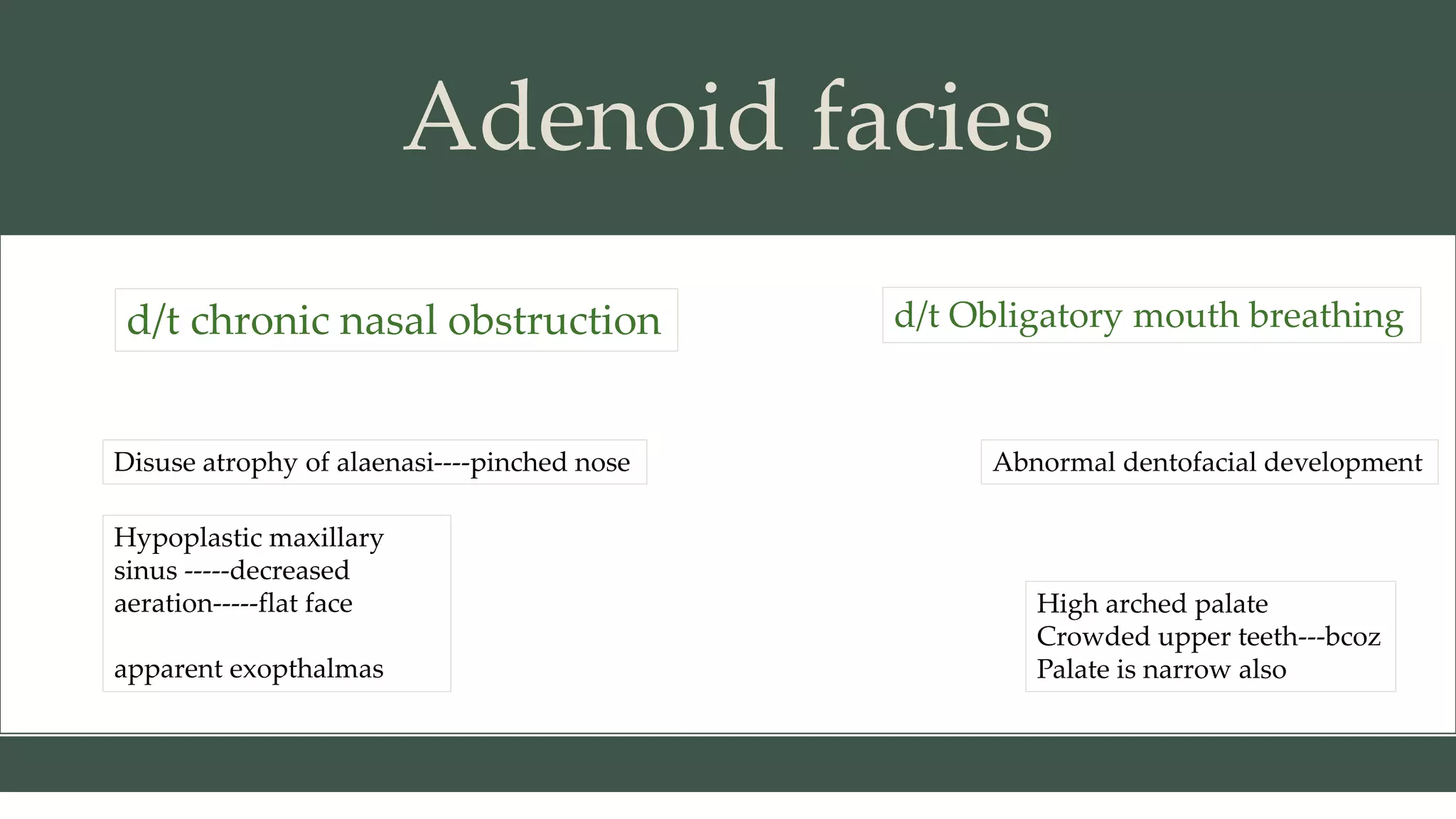
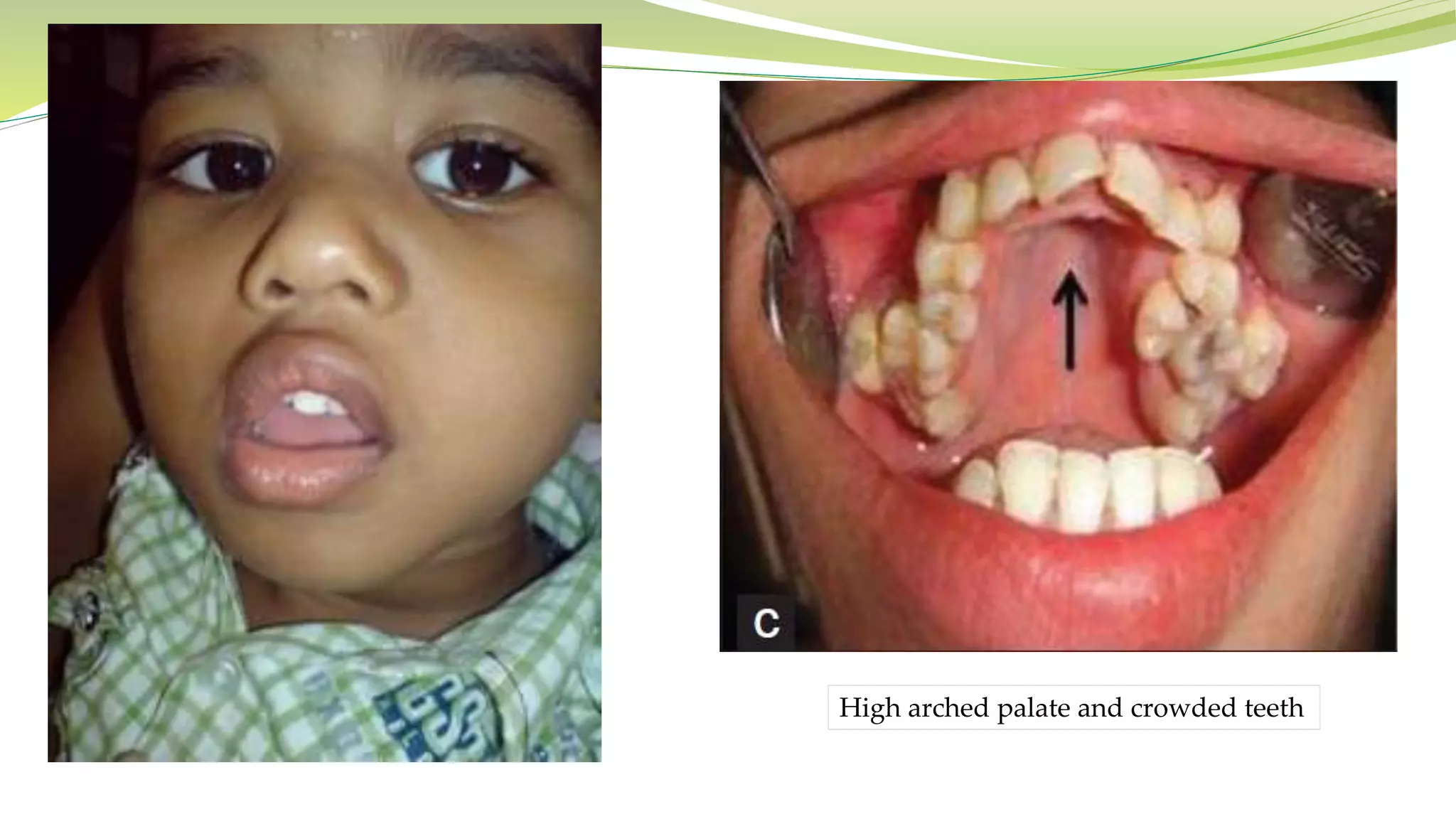
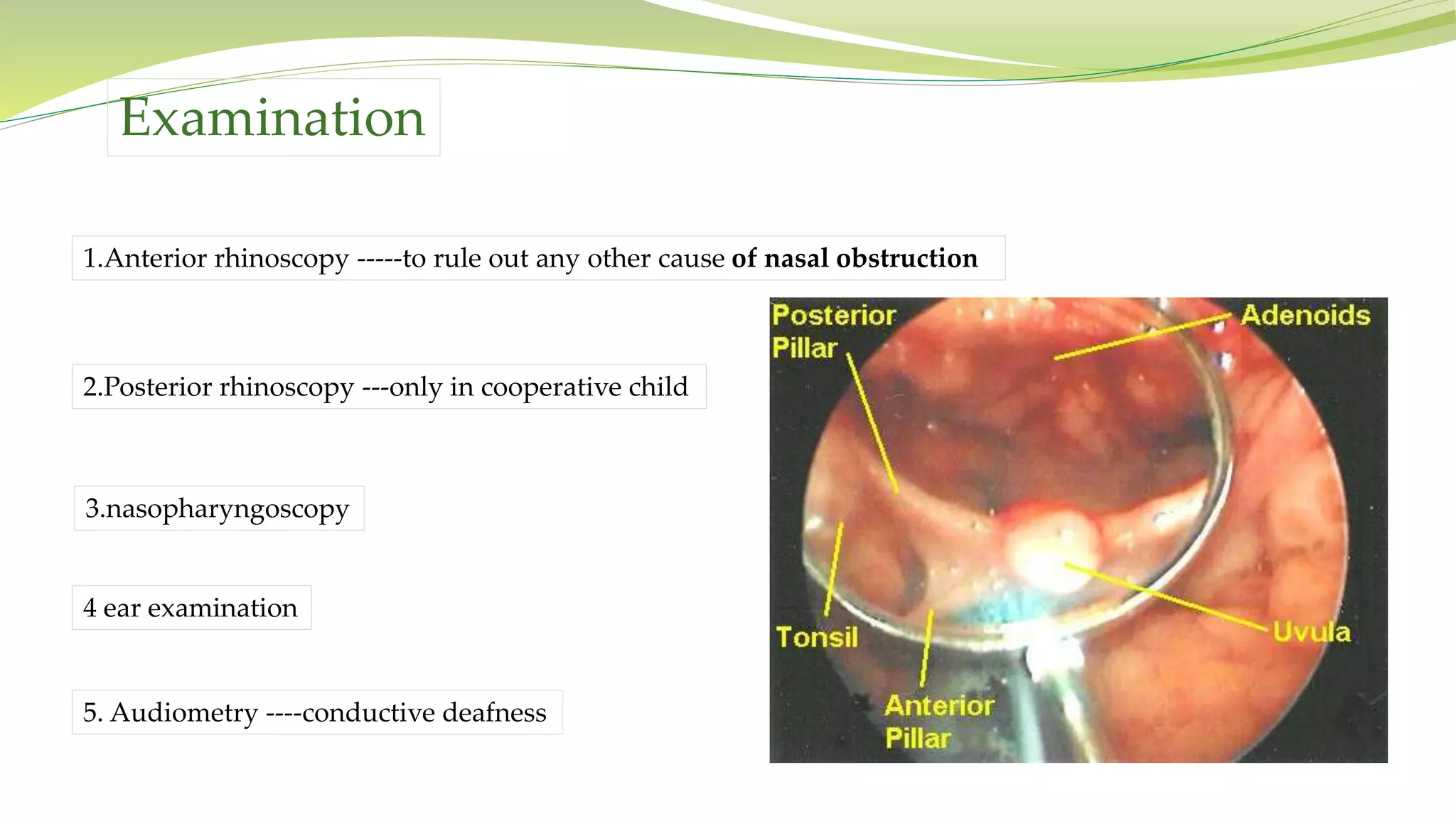
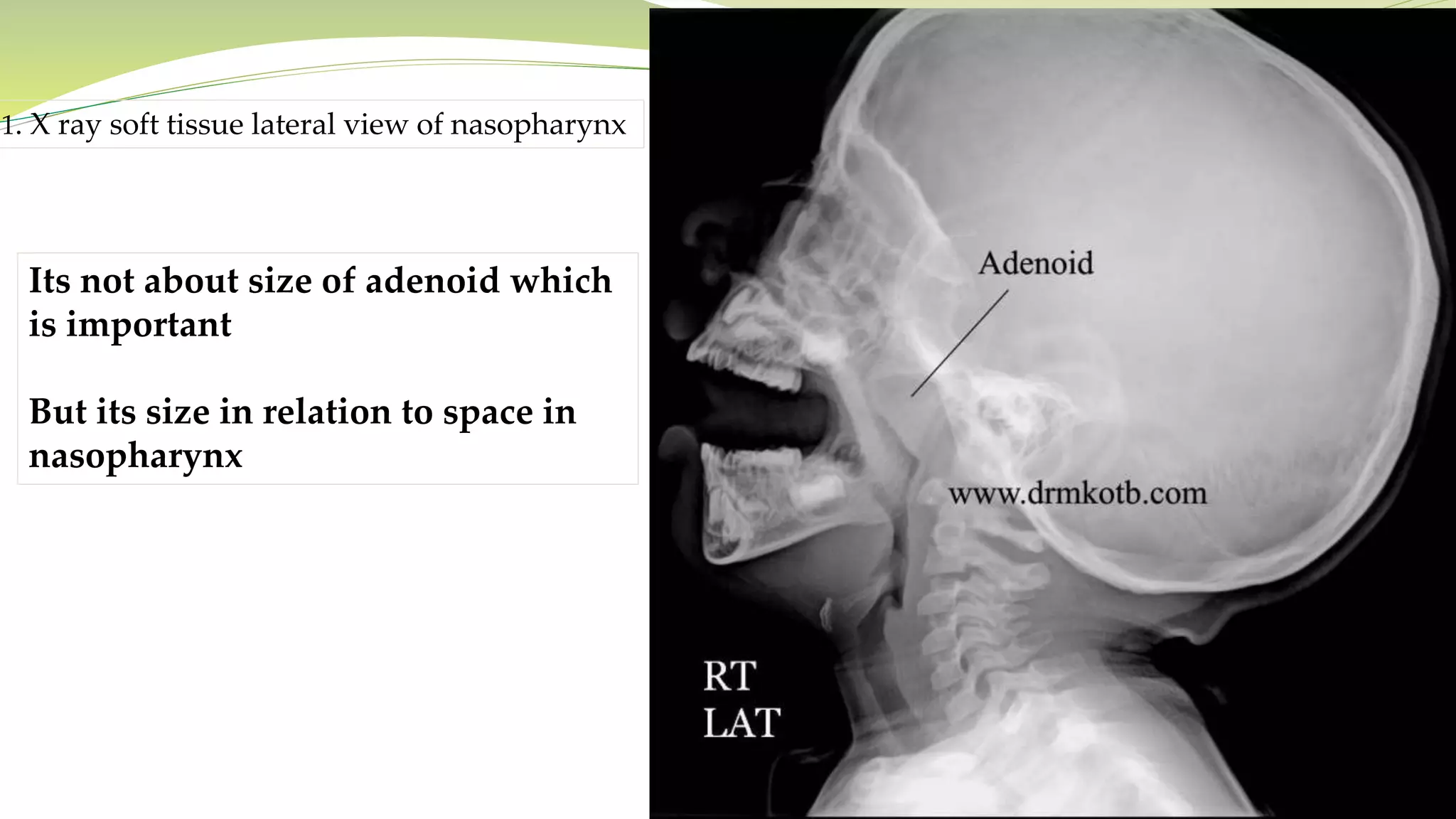
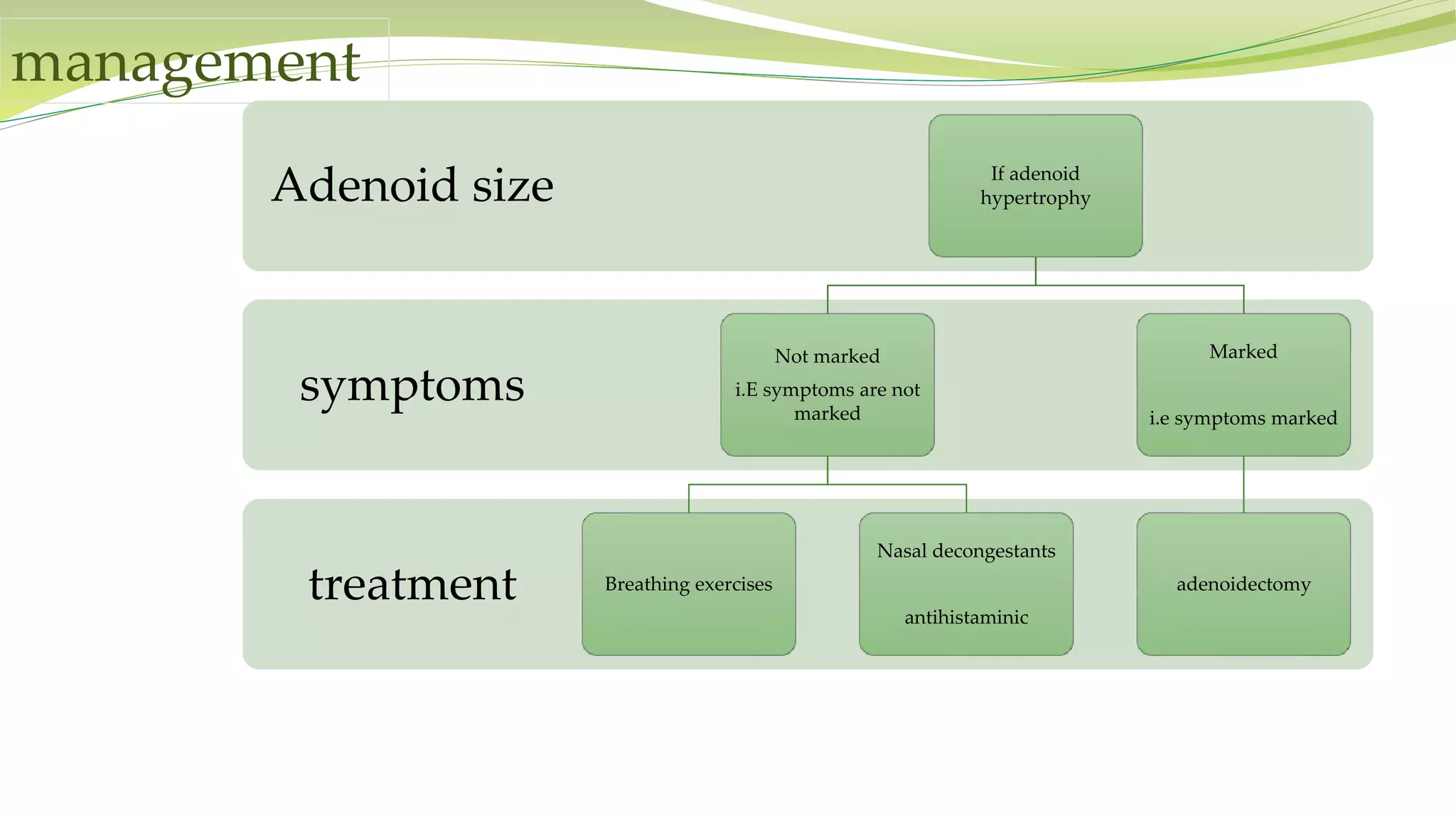
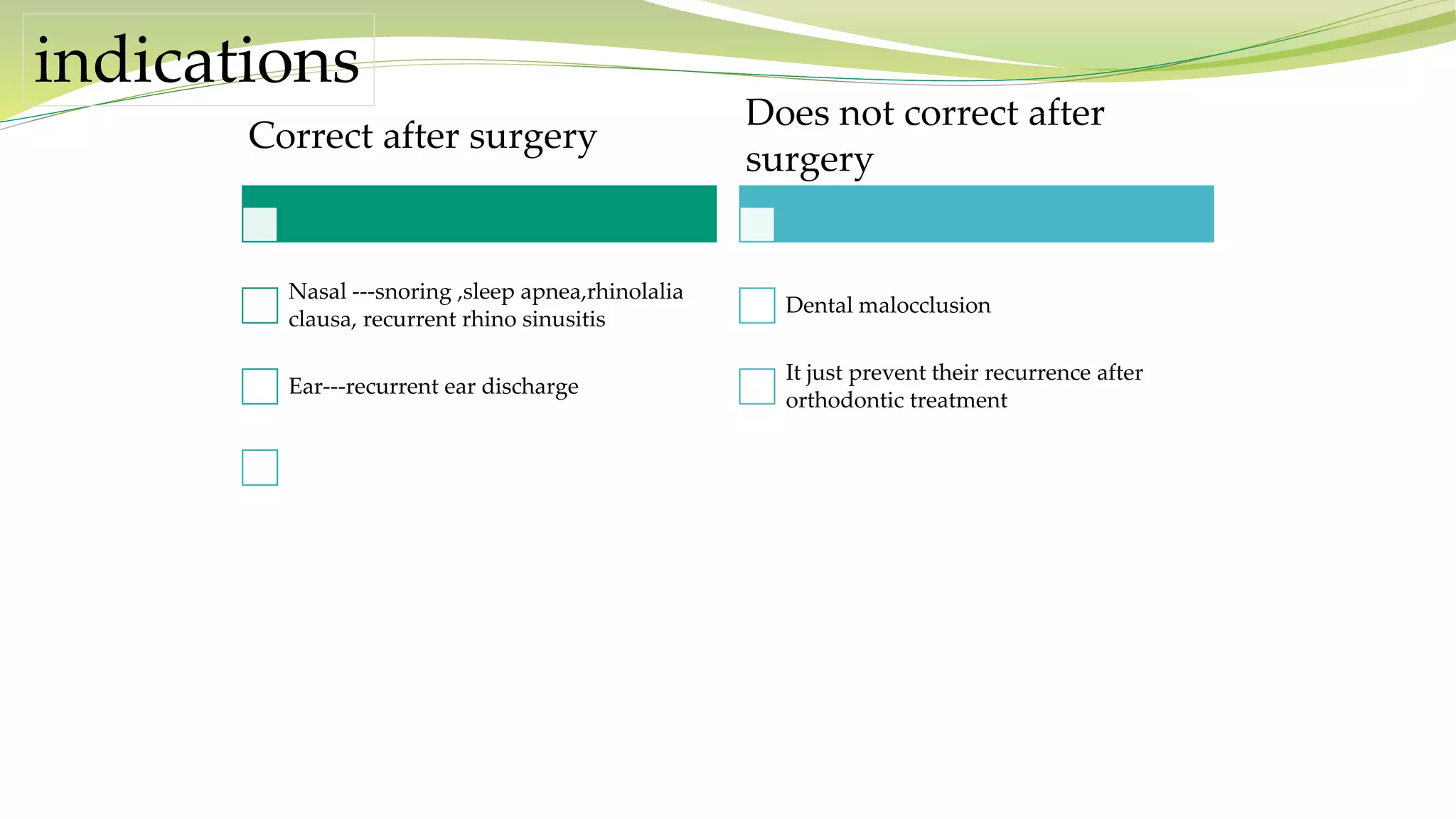
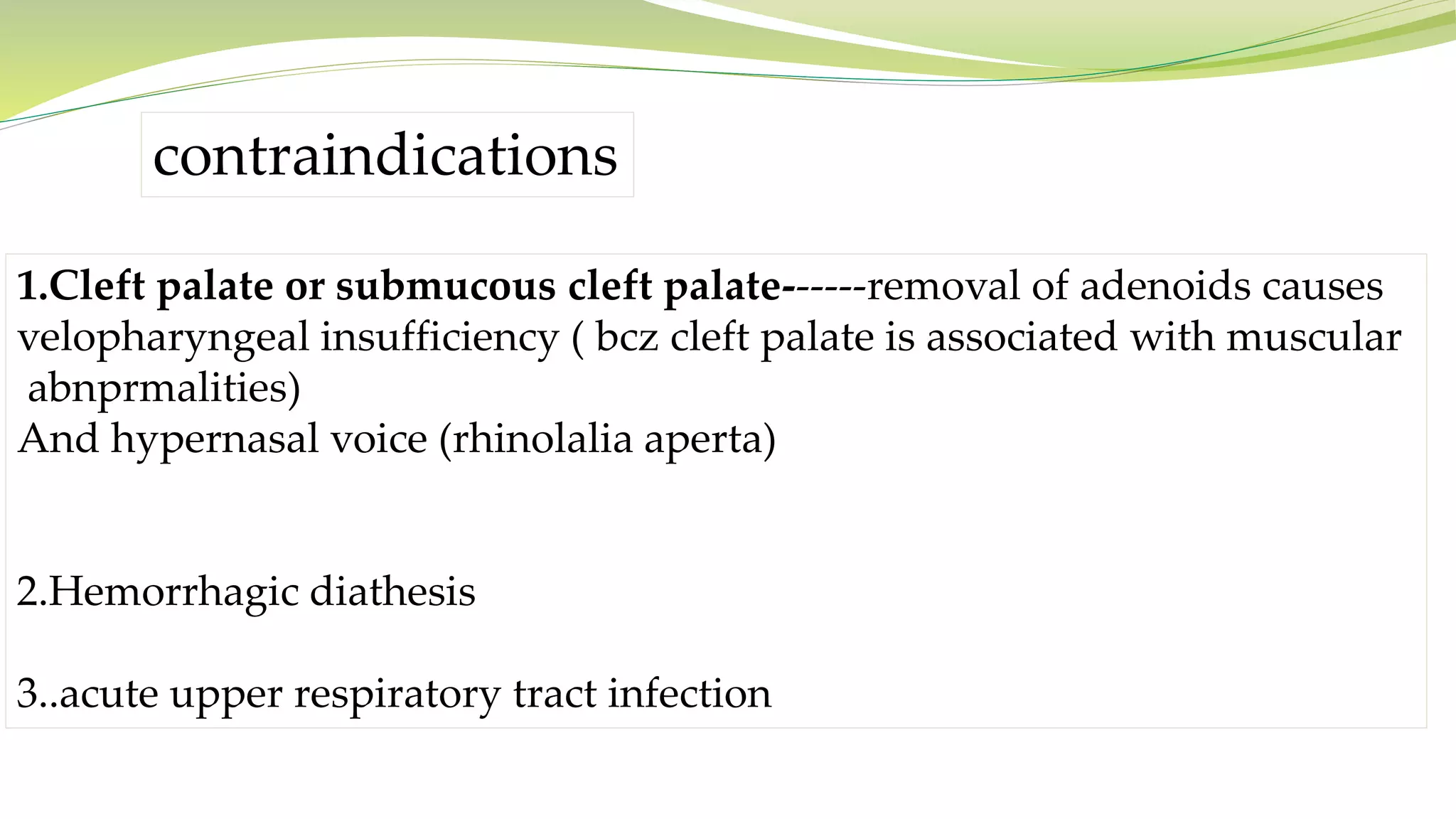
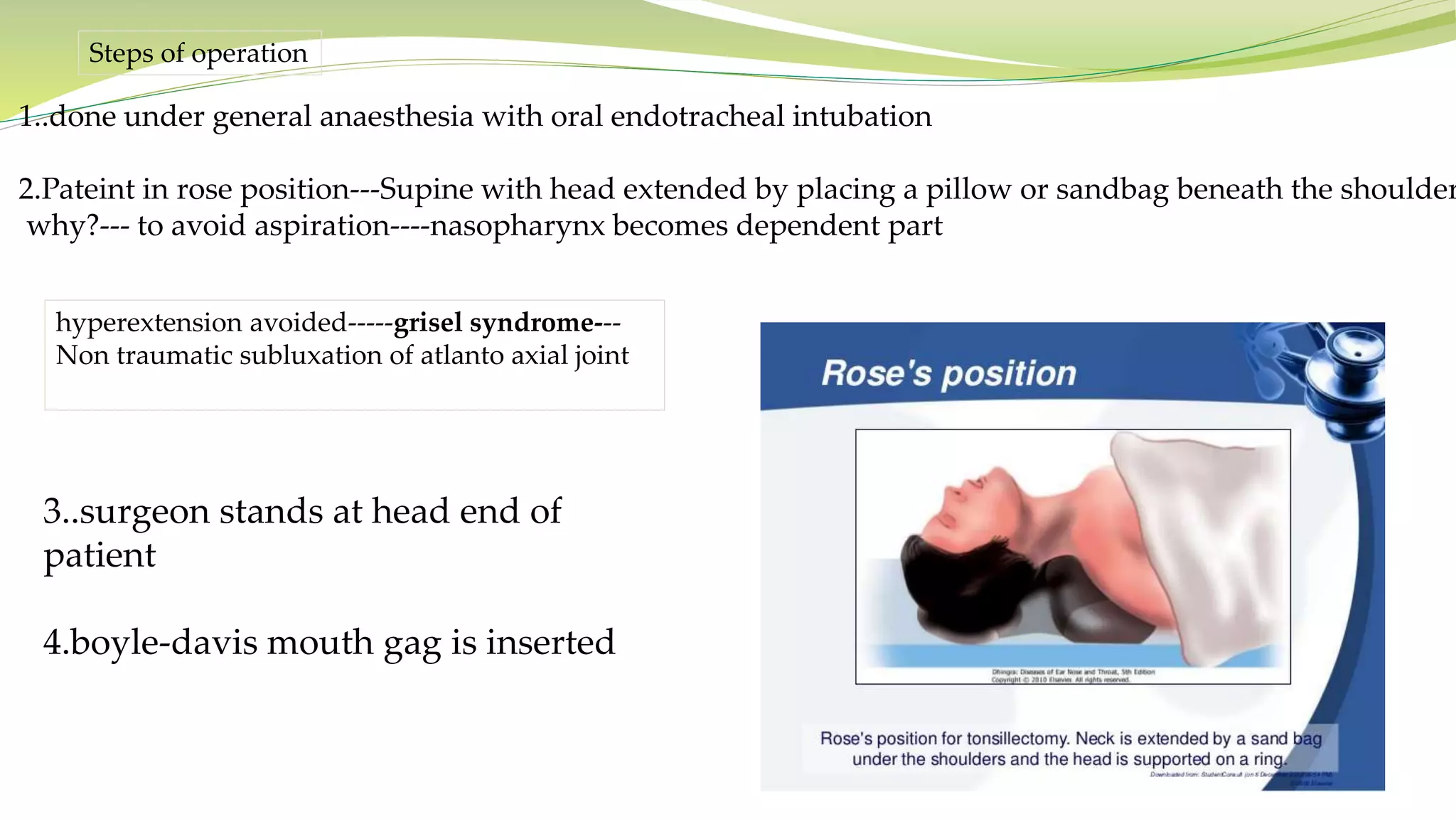
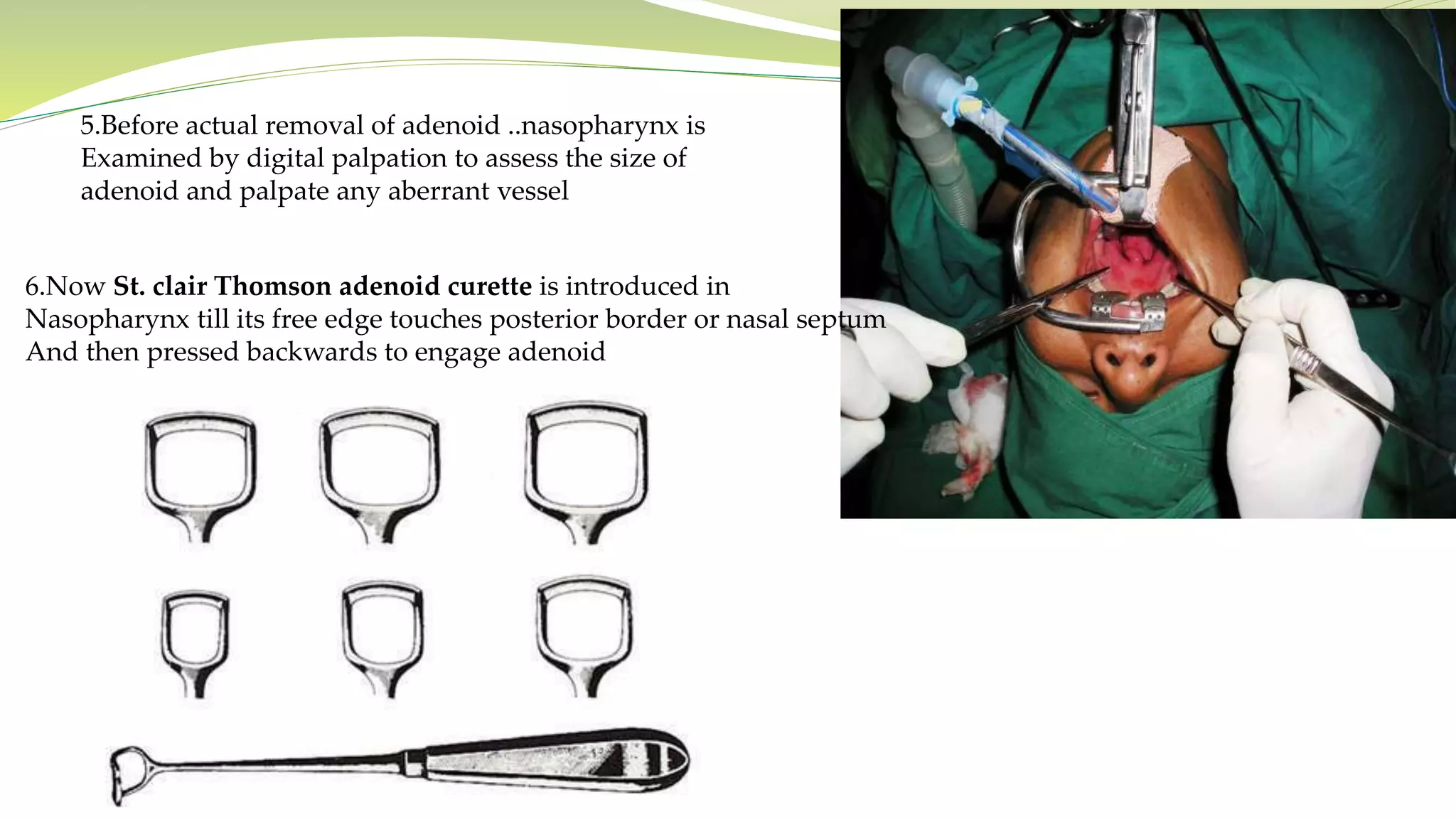
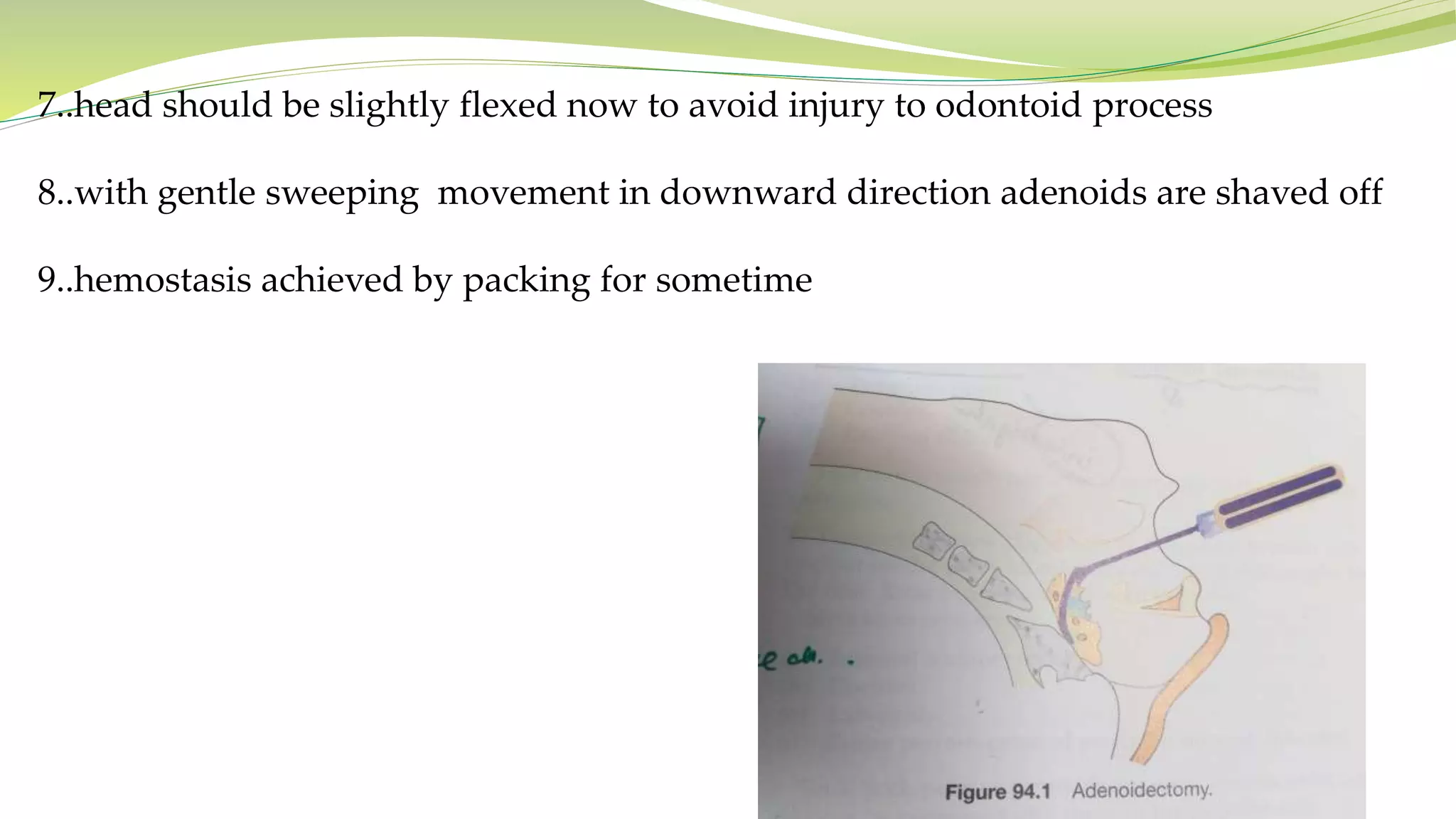


This document provides information about the adenoid, including its anatomy, embryology, blood supply, function, causes of enlargement, presentation of an enlarged adenoid, management, and the procedure for adenoidectomy. Key points: - The adenoid is lymphoid tissue located in the nasopharynx that helps fight infections entering through the nose and mouth. - Enlargement is most common in children under 6 due to frequent infections and immune system stimulation. - Symptoms of an enlarged adenoid include nasal obstruction, ear infections, sleep disturbances, and facial changes. - Treatment involves medications if symptoms are mild or adenoidectomy if symptoms are severe. Adenoidectomy removes























































































