Downloaded 221 times
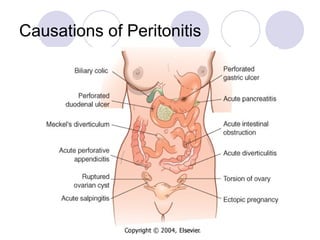
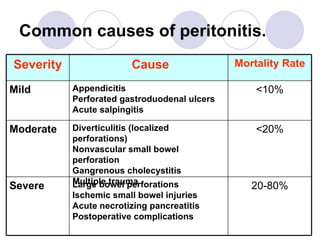
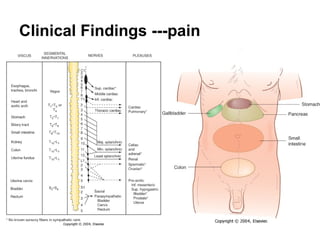
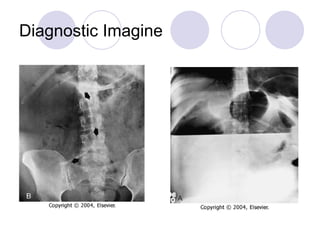
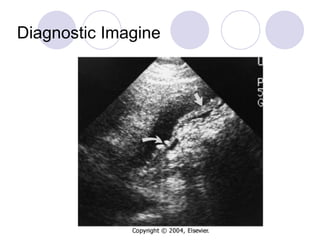
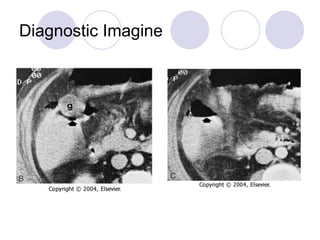
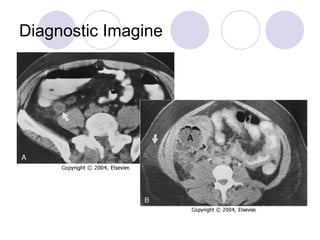

Acute suppurative peritonitis is an inflammatory or infectious response of the peritoneal lining caused by direct irritation or contamination. Common causes include perforations of the large bowel, ischemic small bowel injuries, and acute necrotizing pancreatitis. Clinically, patients present with abdominal pain and tenderness as well as systemic symptoms like fever, chills, and hypotension. Diagnosis is aided by imaging like ultrasound, CT scan, and plain films. Treatment involves preoperative care with IV fluids and antibiotics as well as source control through surgery to remove infected material, correct the underlying cause, and prevent complications.











































































































