+
CLASSIFICATION OF
BACTERIAL PERITONITIS
◼Primarymicrobial peritonitis :occurs when
microbes invade the normally sterile peritoneal cavity via
hematogenous dissemination as infected ascites –peritoneal
dialysis
◼ Secondarymicrobial peritonitis : occurs
subsequenttocontaminationoftheperitonealcavityduetoperforation
orsevereinflammationandinfectionofanintra-abdominalorgan.
Examplesincludeappendicitis,perforationofanyportionofthe
gastrointestinaltract,ordiverticulitis.
◼ Tertiary (persistent) peritonitis: is more
common in immunosuppressed patients (causes see later)
7.
+
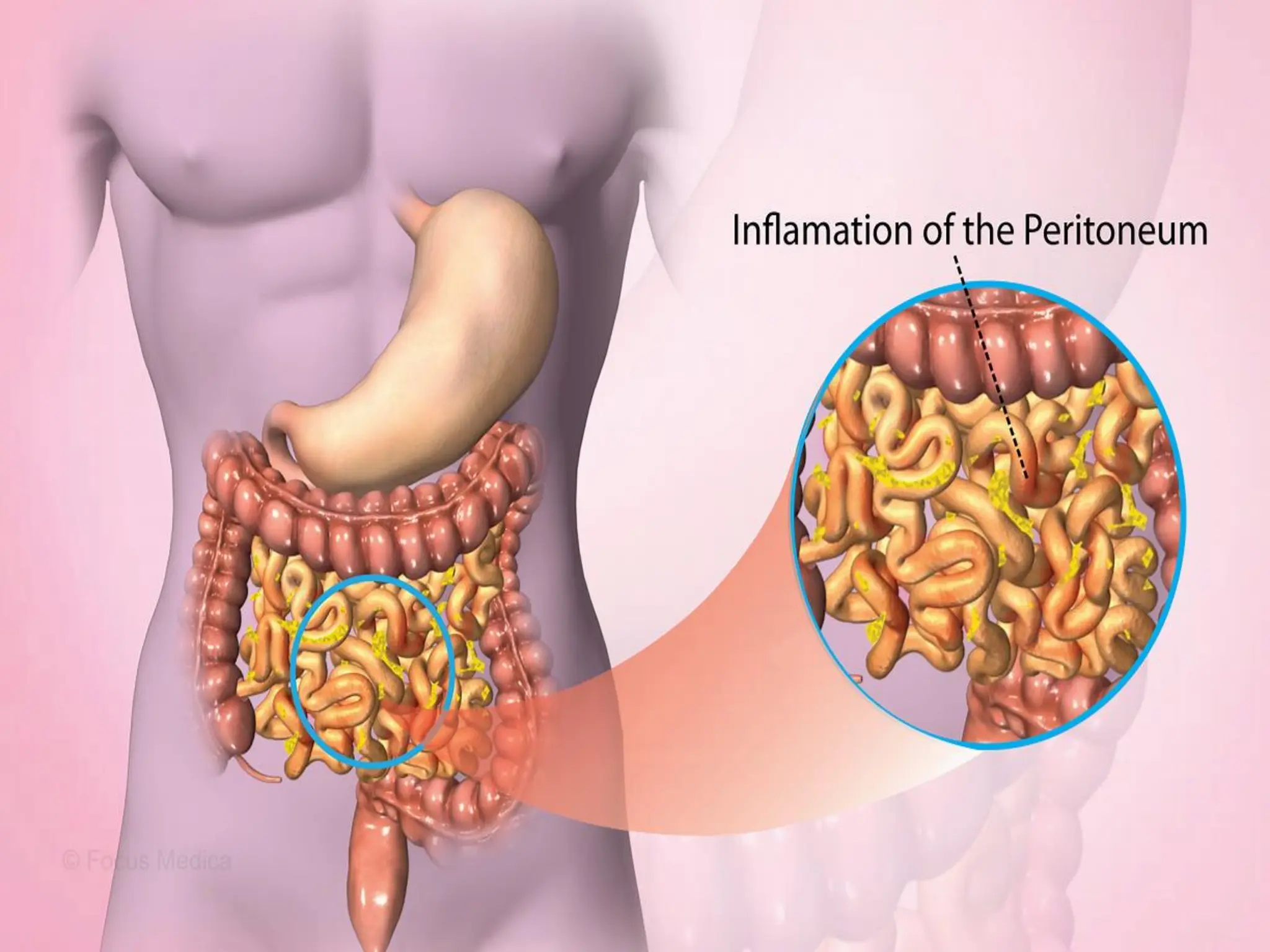
PATHOGENESIS
◼ Release ofhistamine and vasoactive
substances
◼ Creation of inflammatory exudate and
fibrinous adhesions
◼ Release of toxins and consequent toxic
shock
◼ Paralytic ileus complicate the condition
9.
+
PATHOLOGICAL TYPES
◼ Localisedperitonitis
◼ Anatomical
◼ Pathological
◼ Diffuse (generalised) peritonitis
◼ Speed of peritoneal contamination(failure of localization)
◼ Stimulation of peristalsis(food or even water)
◼ The virulence of the infecting organism
◼ Youngchildren havea small omentum
◼ Disruption of localised collections(appendix mass or pericolic abscess)
◼ Deficient naturalresistance
10.
+
CLINICAL FEATURES
Localised peritonitis
◼Localised guarding
◼ Rebound tenderness
◼ Rigidity
◼ The pain is referred to the C5 dermatome(sub
phernic)
◼ Pelvic peritonitis; rectal or vaginal
examination marked tenderness
11.
+
DIFFUSE (GENERALISED)
PERITONITIS
EARLY
◼ Abdominalpain is severe and made worse by
moving or breathing; experienced at the site of the
spreads outwards from this
original lesion and
point.
◼ The patient usually lies still. Tenderness and
generalised guarding are found on palpation.
◼ Infrequent bowel sounds may still be heard but
they cease with the onset of paralytic ileus.
◼ Pulse and temperature rise in accord with degree of
inflammation and infection.
12.
+
DIFFUSE (GENERALISED)
PERITONITIS
LATE
◼ Generalisedrigidity
◼ Distension and absent bowel sounds
◼ Circulatory failure ensues, with cold, clammy
extremities
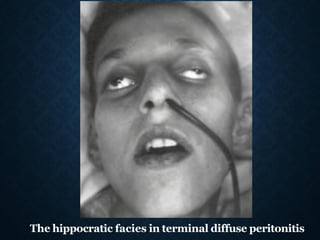
◼ Sunken eyes, dry tongue, thready (irregular)
pulse, and drawn and anxious face (hippocratic
facies)
◼ The patient finally lapses into unconsciousness
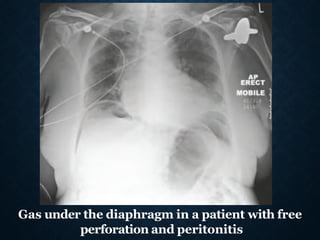
Gas under thediaphragm in a patient with free
perforation and peritonitis
17.
+
MANAGEMENT
General care ofthe patient
◼ Correction of fluid loss and circulating
volume
◼ Urinary catheterisation ± gastro-
intestinal decompression(NG tube)
◼ Antibiotic therapy
◼ Analgesia
18.
+
MANAGEMENT
• Specific treatmentof the cause
◼Non-surgical treatment is preferred
◼Surgery is directed to removing (or
diverting) the cause and subsequent
adequate peritoneal lavage ± drainage
◼The whole peritoneal cavity be explored
and mopped. The use of a large volume
of saline (typically 3 litres) containing
dissolved antiseptic or antibiotic
+ ABDOMINAL
COMPLICATIONS OF
PERITONITIS
◼Paralytic ileus
◼ Residual or recurrent
abscess/inflammatory mass
◼ Portal pyaemia/liver abscess
◼ Adhesional small bowel
obstruction
21.
+ SPECIAL FORMSOF PERITONITIS
operations/
Bile peritonitis
◼ Perforated gall bladder
◼ Post-cholecystectomy
◼ Following other
procedures:
◼Blunt or penetrating hepatobiliary or
duodenal trauma
22.
+ SPECIAL FORMSOF PERITONITIS
Tuberculous peritonitis
◼ Acute (may be clinically indistinguishable from
acute bacterial peritonitis) and chronic forms
◼ Abdominal pain, sweats, malaise and weight
loss
◼ Ascites common, may be loculated
◼ Caseating peritoneal nodules – distinguish from
metastatic carcinoma and fat necrosis of
pancreatitis
◼ Intestinal obstruction may respond to anti-
tuberculous treatment without surgery
23.
+ SPECIAL FORMSOF PERITONITIS
Familial Mediterranean fever (periodic
peritonitis)
◼ Comes in attacks
◼ Recurrentwith remissions and
exacerbations
◼ Plus pain in the thorax and joints
◼ Familial Female more,children more
◼ +ve appendectomy
◼ Colchicine therapy
24.
+ SPECIAL FORMSOF PERITONITIS
INTRAPERITONEAL ABSCESS
Symptoms
◼ Malaise, lethargy – failure to recover from
surgery as expected
◼ Anorexia and weight loss
◼ Sweats ± rigors
◼ Abdominal/pelvic pain
◼ Symptomsfrom local irritation
25.
+ SPECIAL FORMSOF PERITONITIS
Signs
◼Increased temperatureand pulse ±
swinging pyrexia
◼Localised abdominal tenderness ±
mass (including on pelvic exam)
26.
+
TERTIARY PERITONITIS ISMAINLY:
A. Postoperative complication of
delayed diagnosis of secondary
peritonitis
poly
B. Residual intraperitoneal abscess
C. Wrong management of
traumatized patient
D. Usually occurred in ascetic patents
with hepatorenal impairment
27.
+
IN
SUMMARY
❑Peritonitis is avery common serious
surgical emergency
❑Early effective Treatment is the cornerstone
❑Treatment underlying cause and
complications