Download as PPSX, PPTX
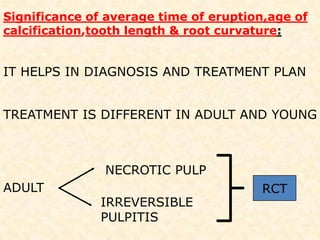
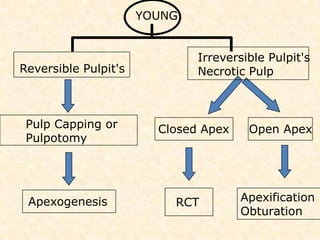
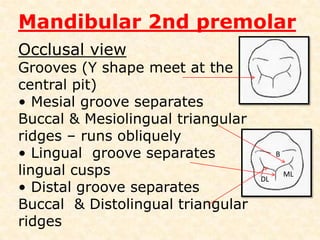
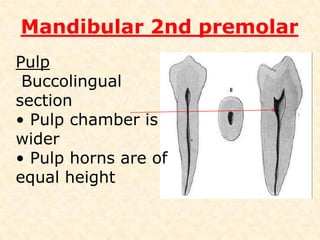
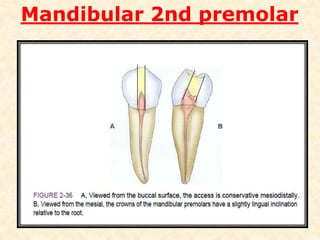
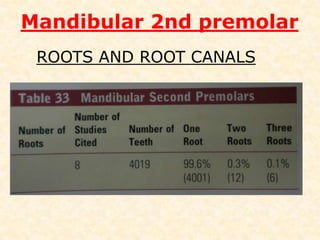
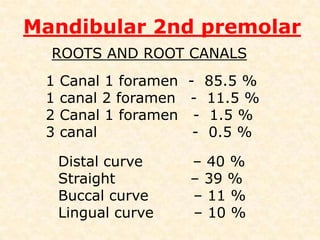
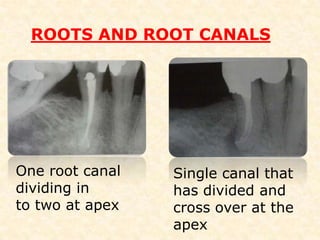
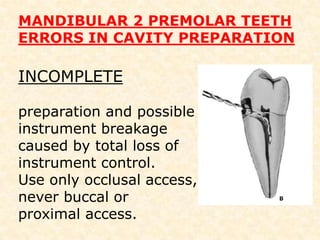
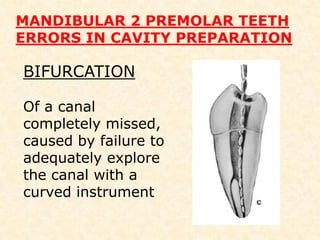
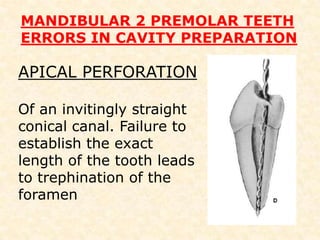
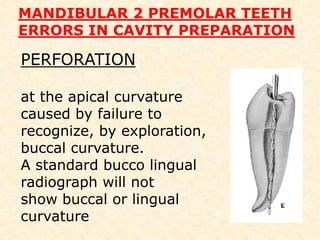
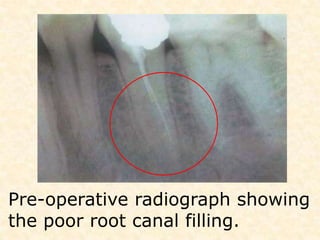
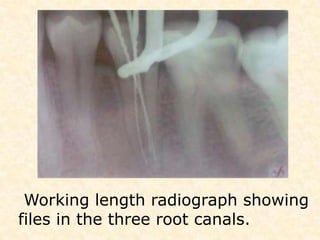

This document provides information about the anatomy and root canal treatment of the mandibular second premolar tooth. It describes the external and internal anatomy of the tooth, including average measurements, root canal morphology, and anatomical variations that may be present. It also discusses errors that can occur during root canal treatment of this tooth and provides a case example of successfully treating a mandibular second premolar with three root canals.

















![]Dental Occlusion part 1](https://cdn.slidesharecdn.com/ss_thumbnails/occlusionpart1-160420073612-thumbnail.jpg?width=640&height=640&fit=bounds)
























![dental_anatomy_gggggttgttttyyroup_1_45[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dentalanatomygroup1451-240609100908-80bf70c3-thumbnail.jpg?width=640&height=640&fit=bounds)










