
Downloaded 1,065 times

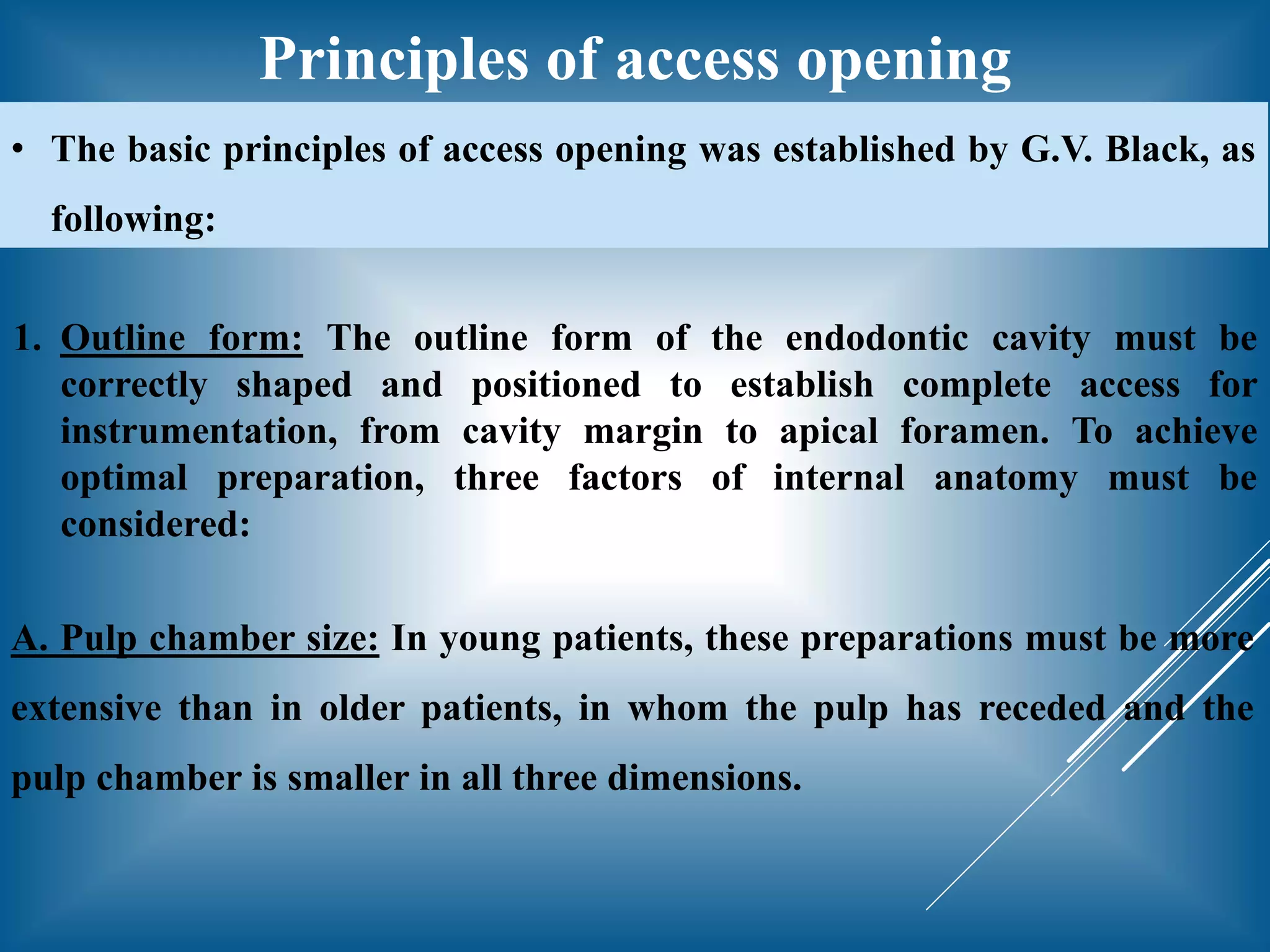
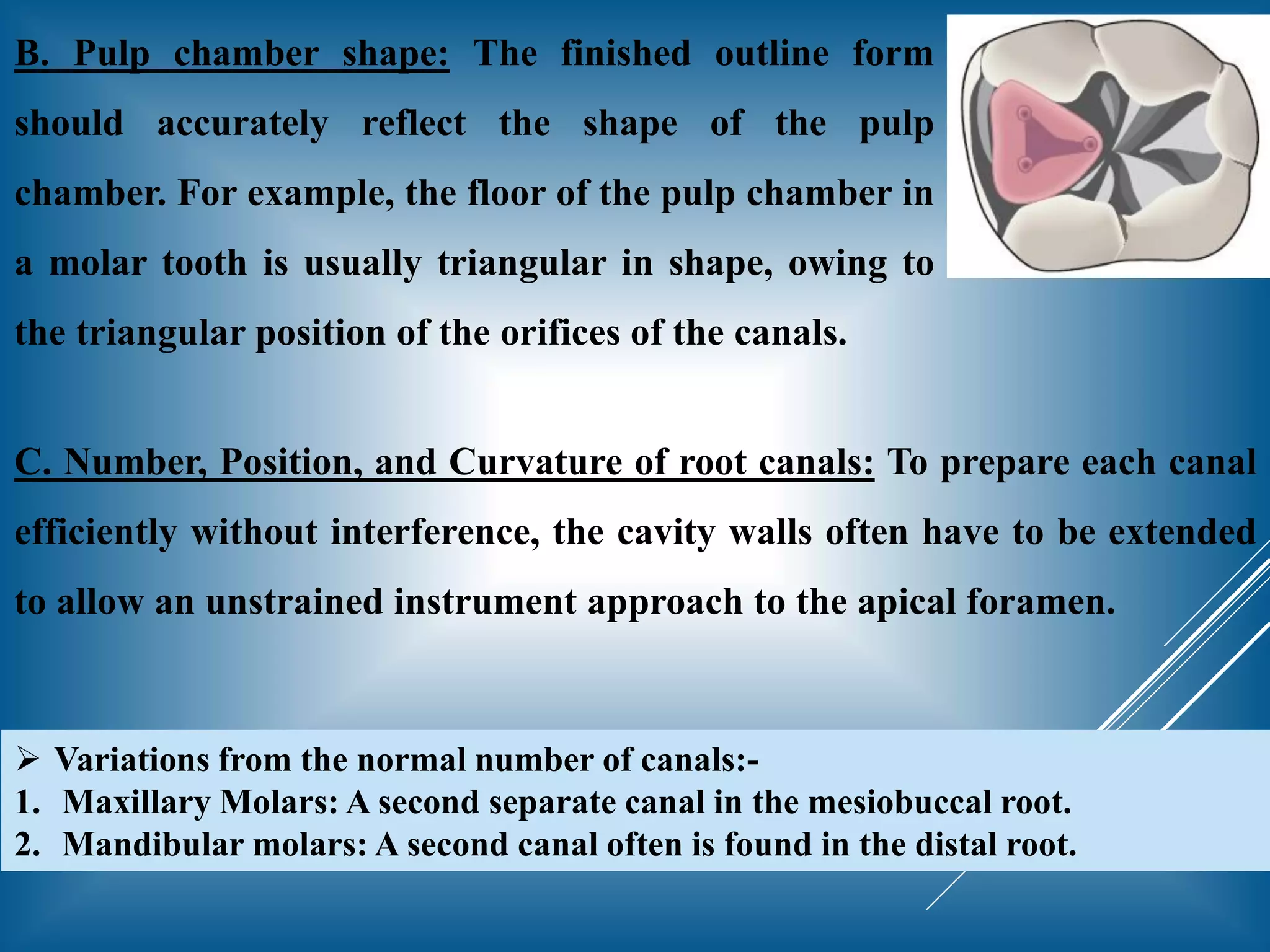
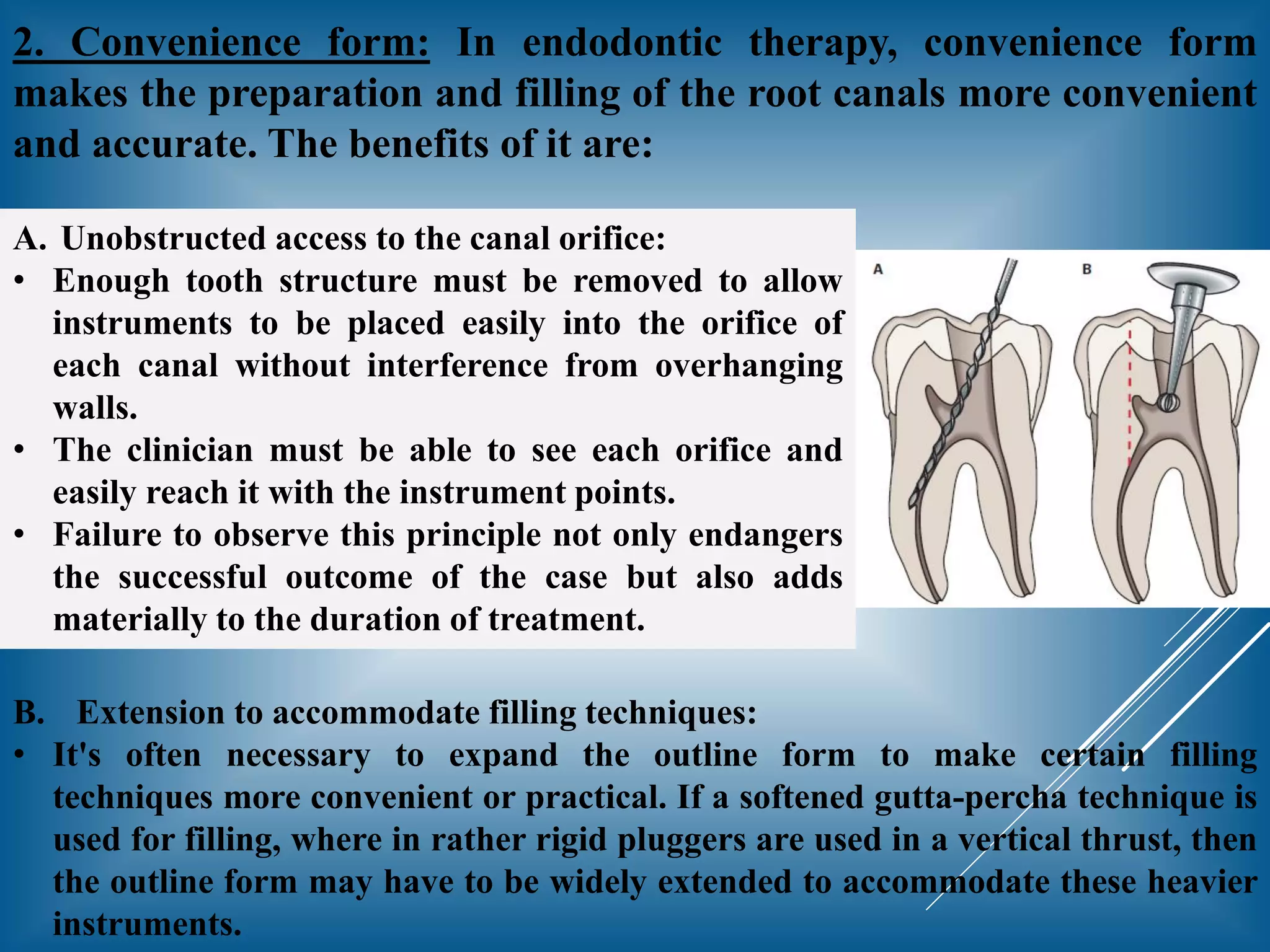
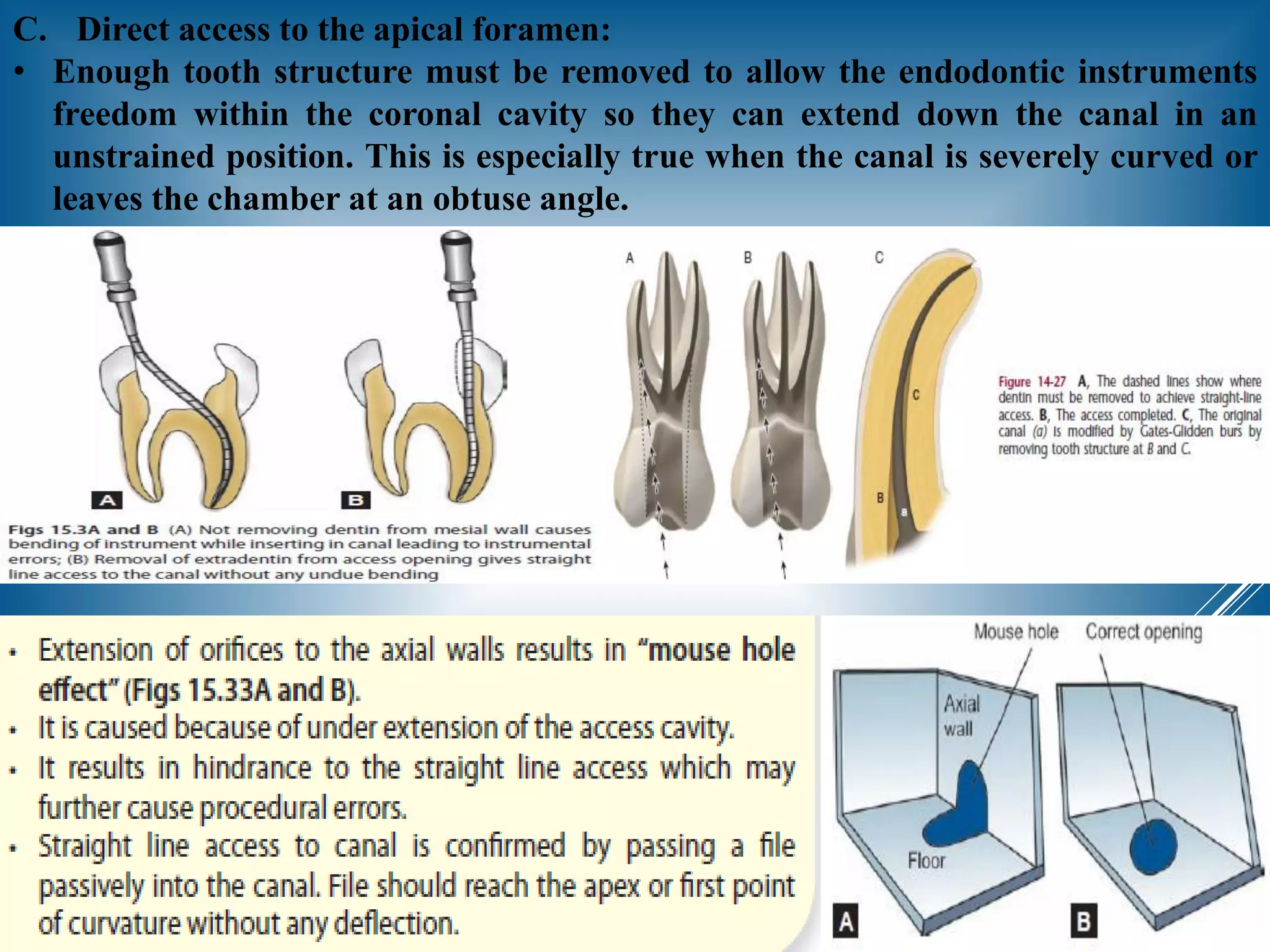

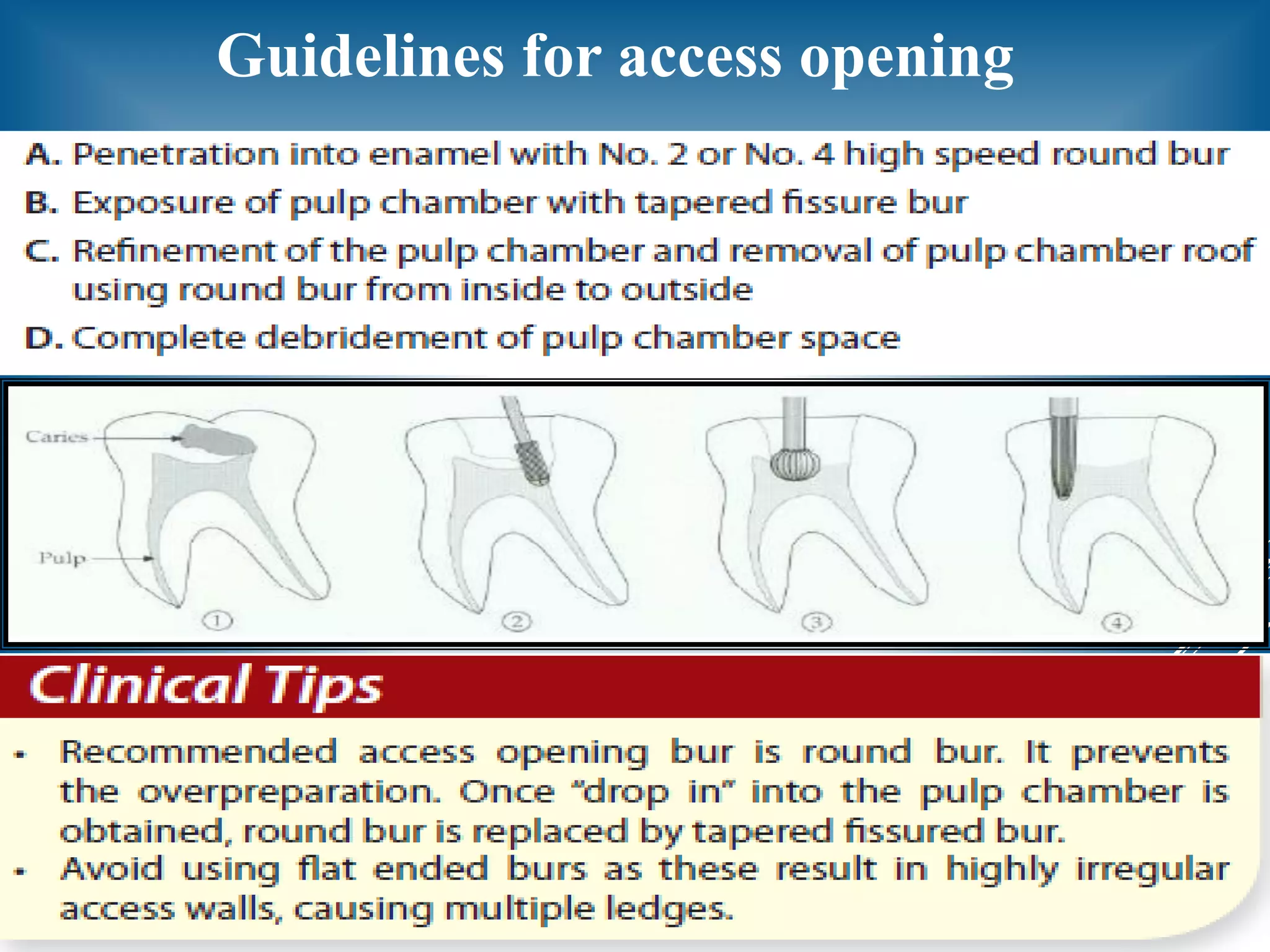
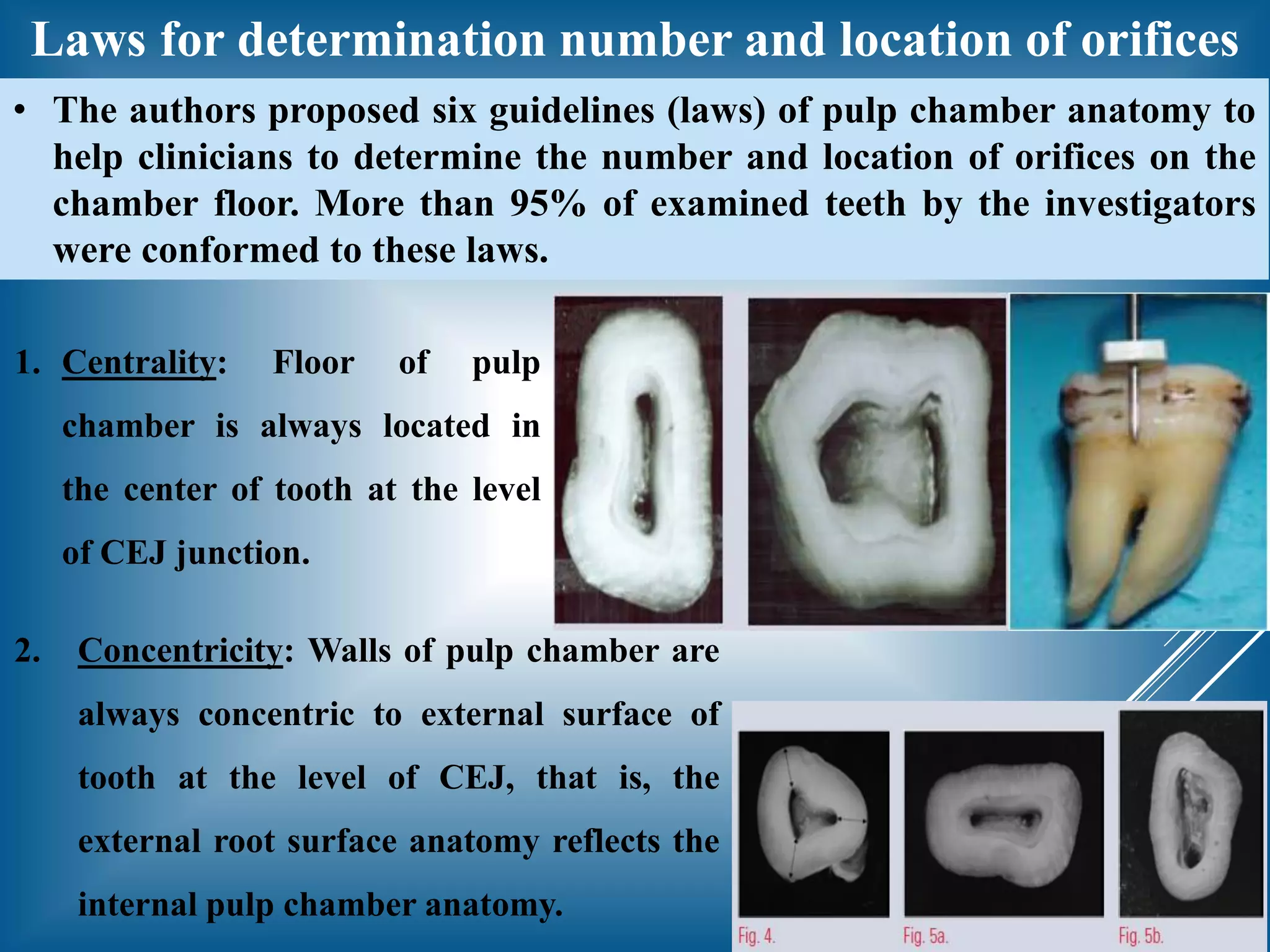
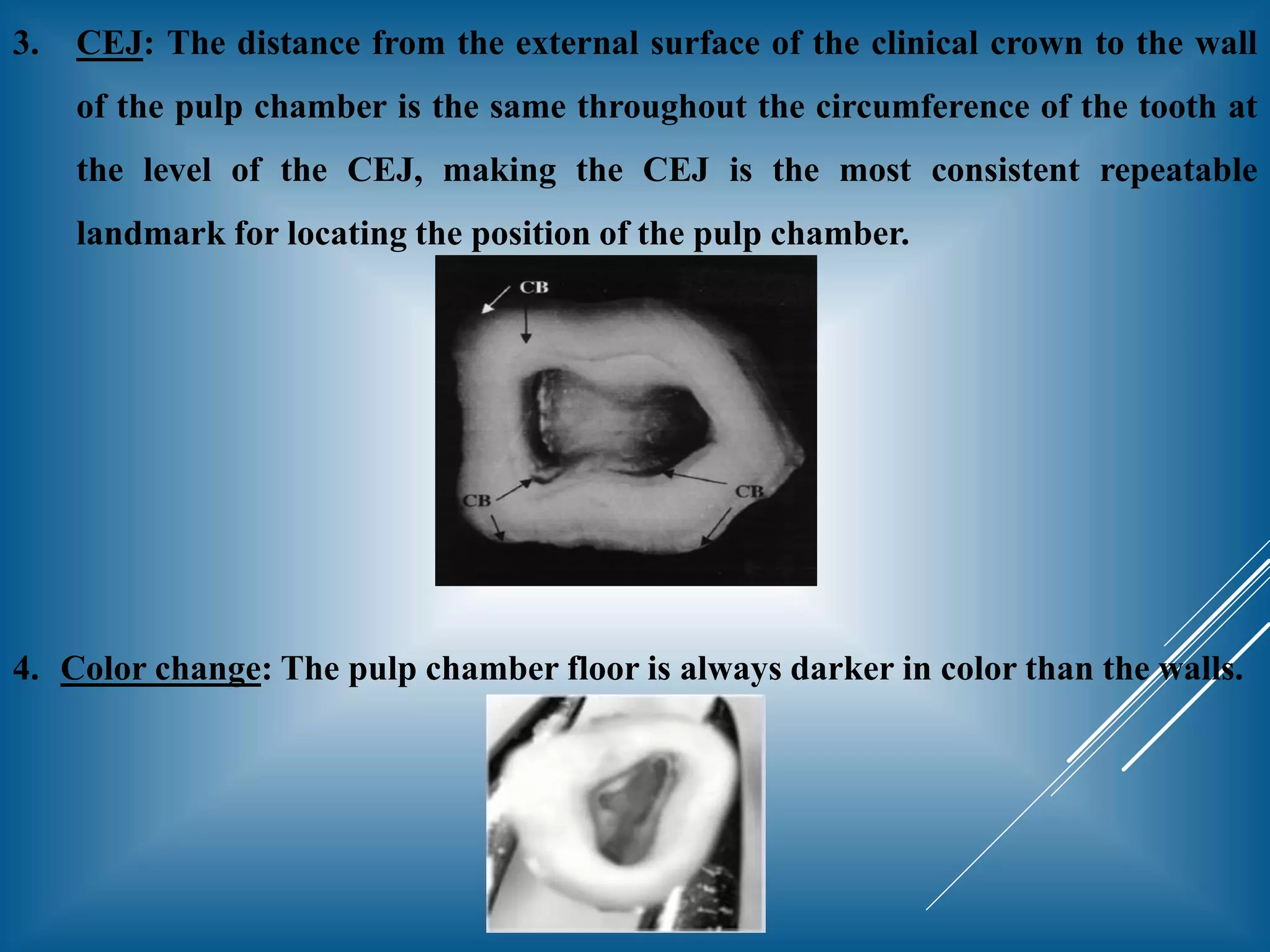
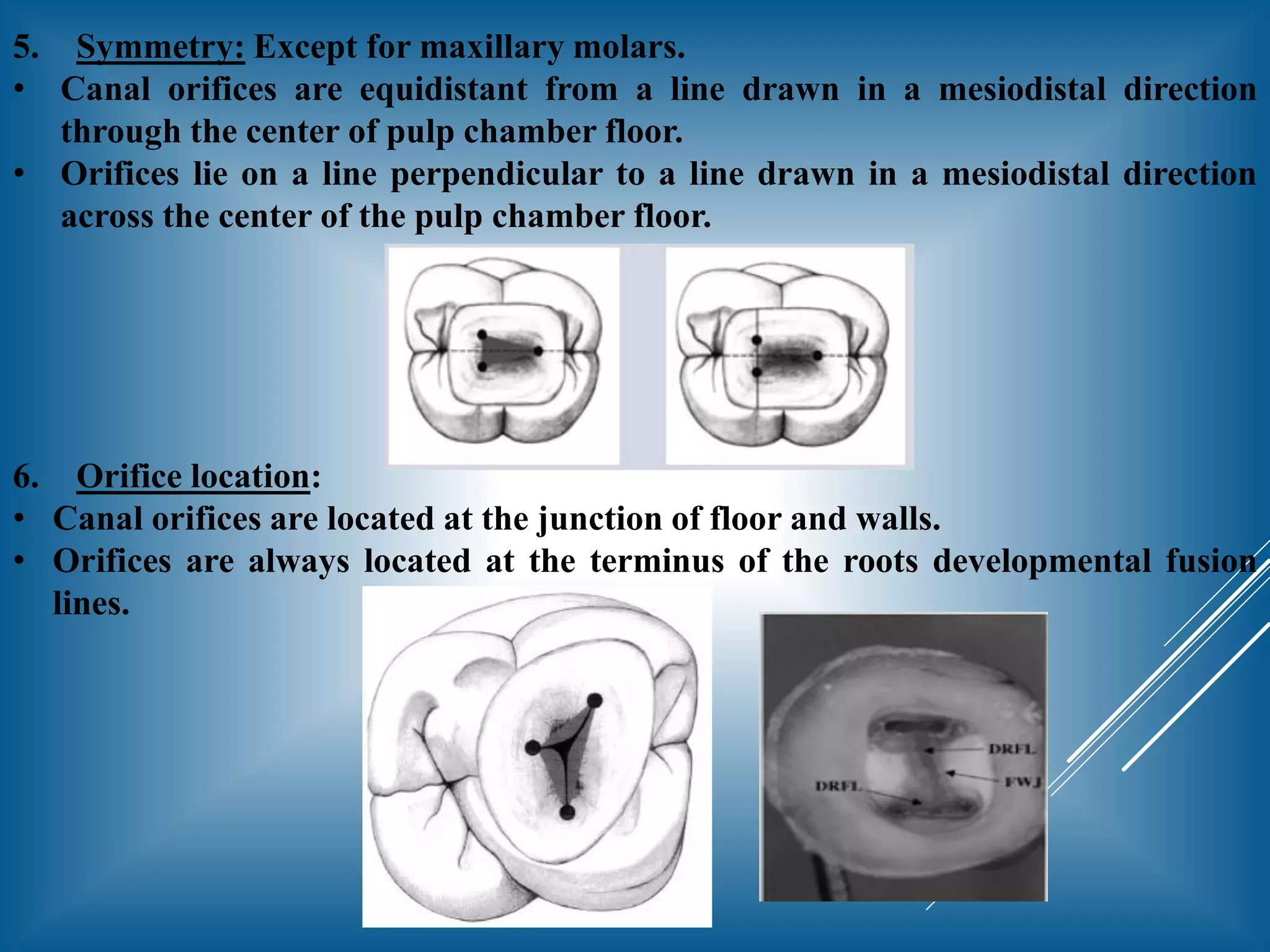





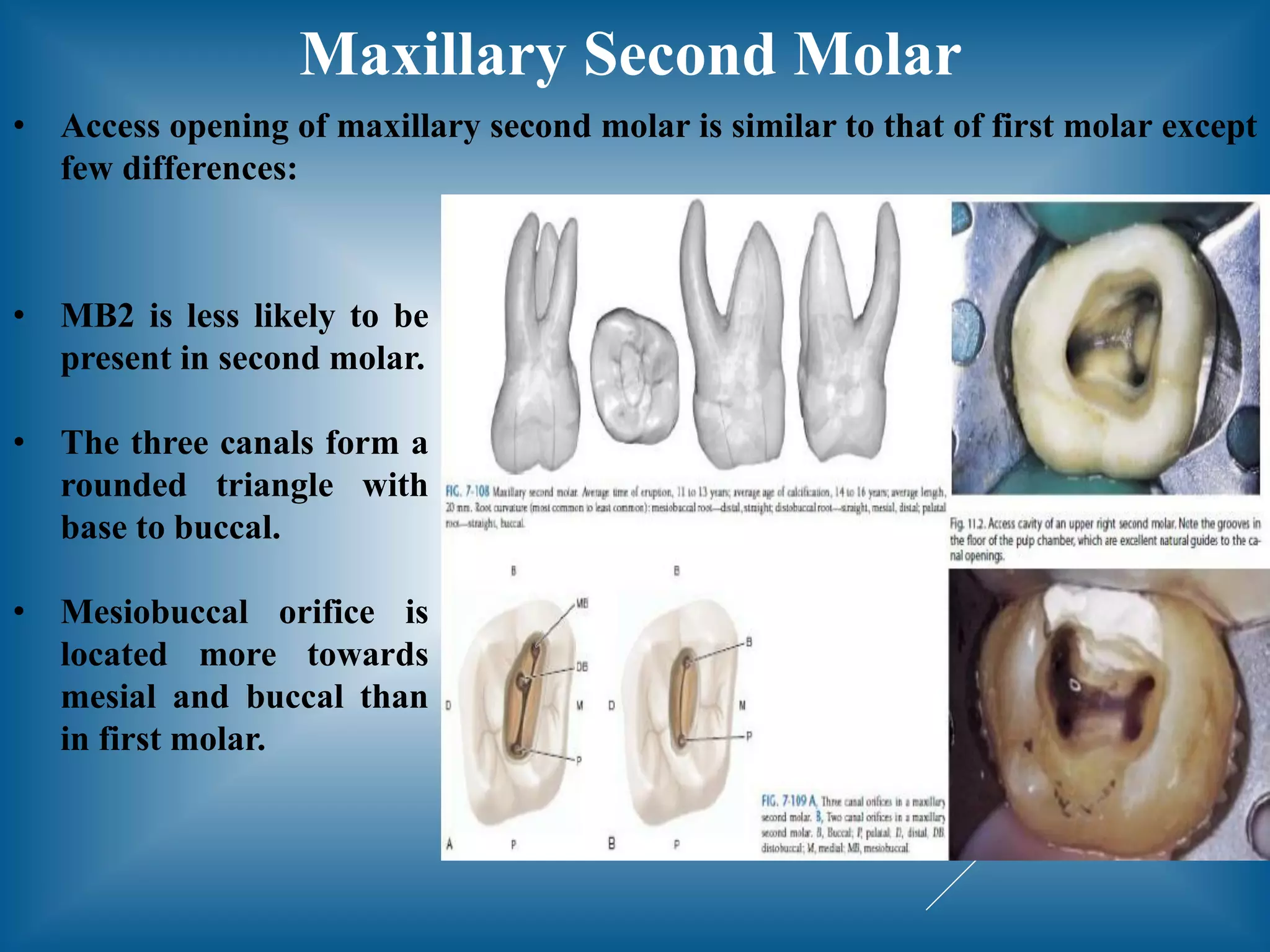

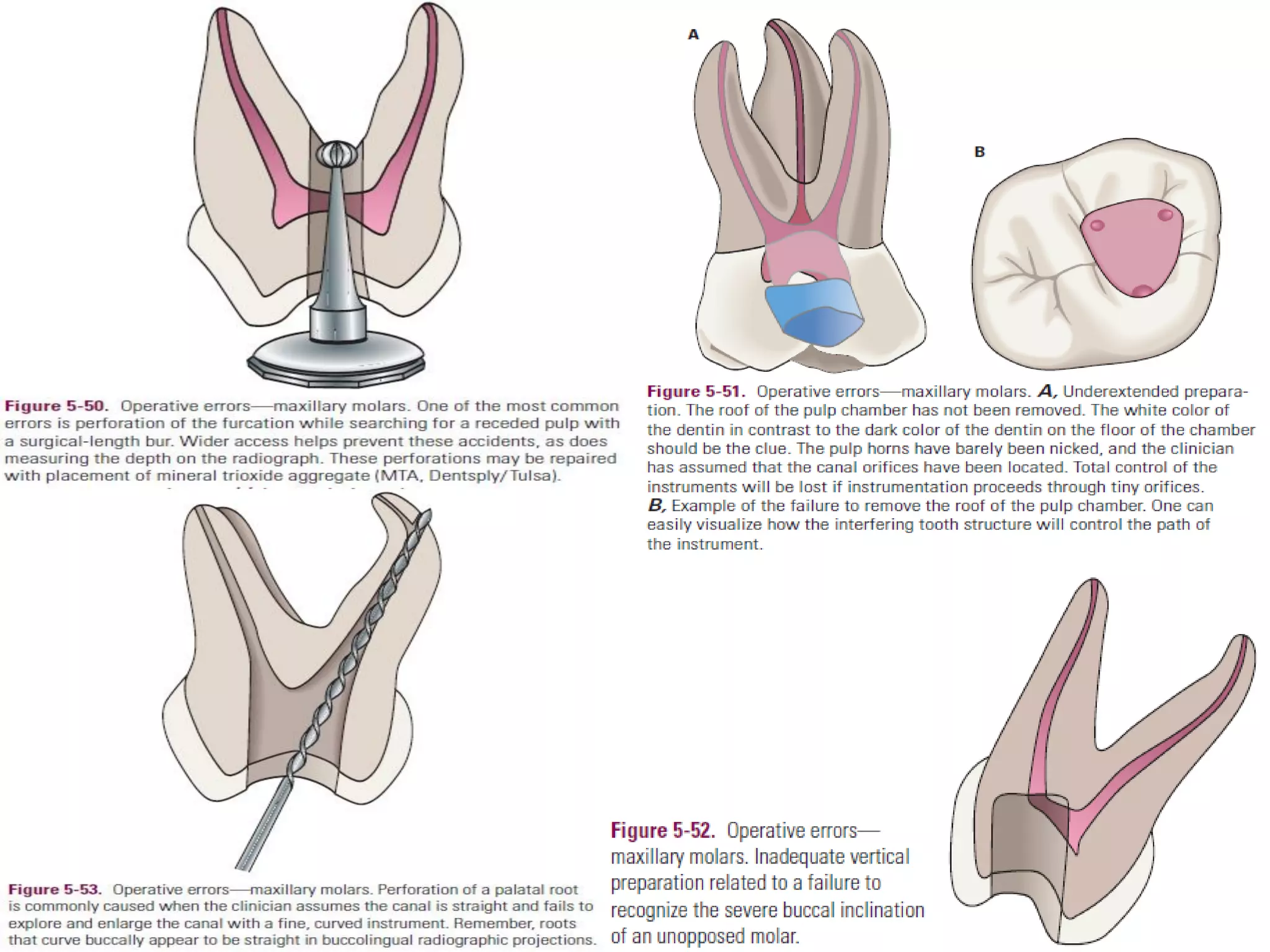





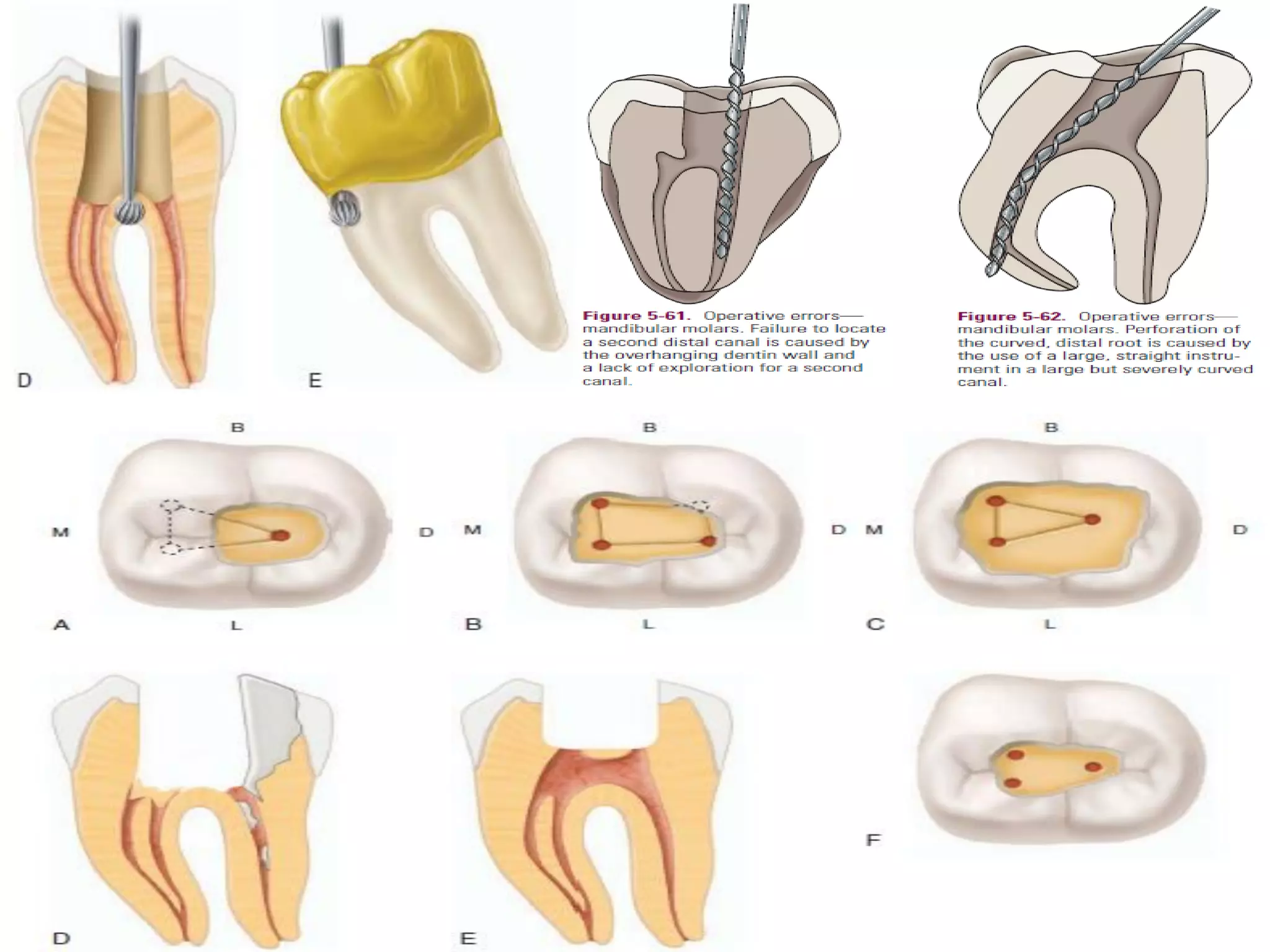
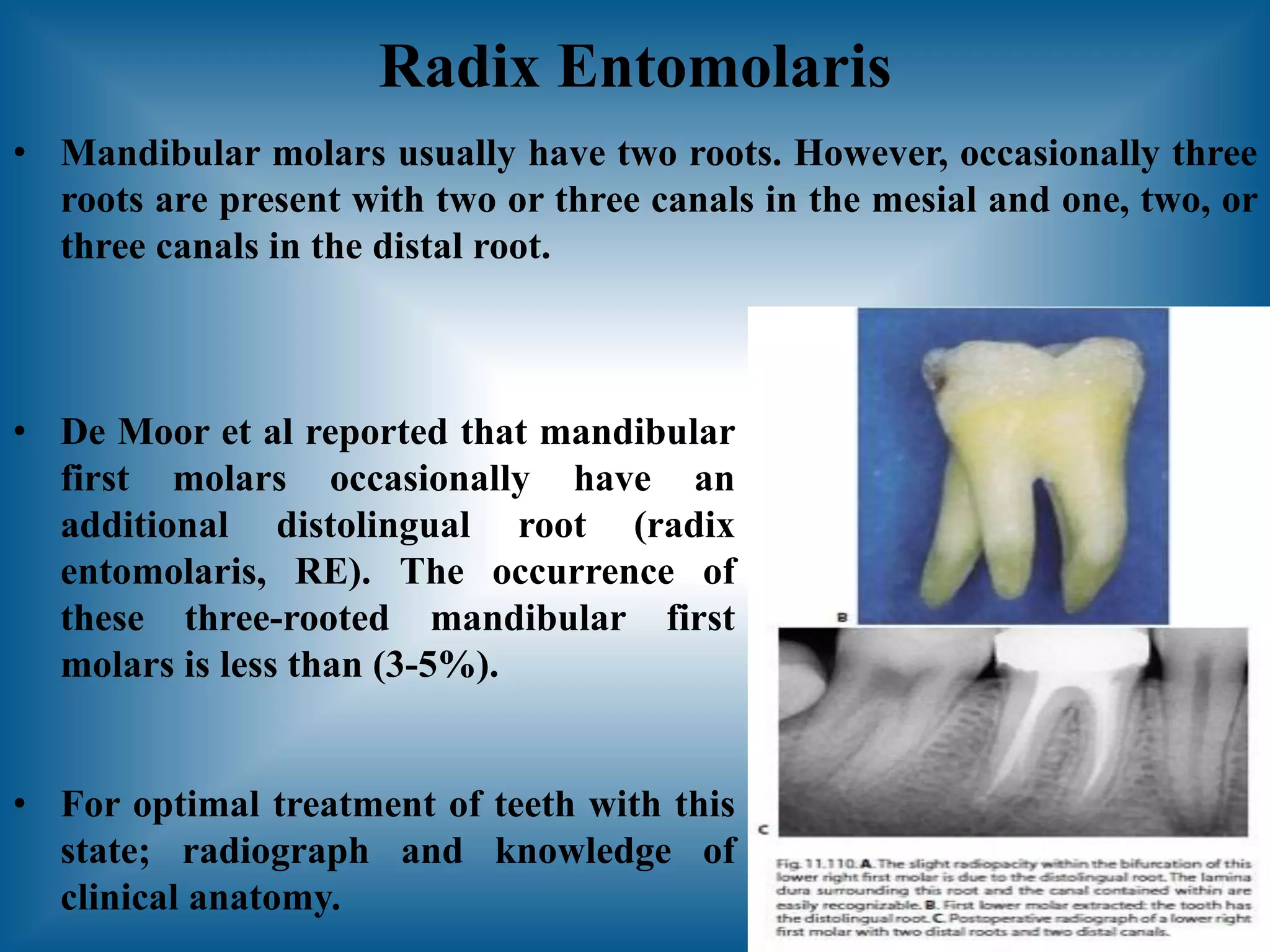
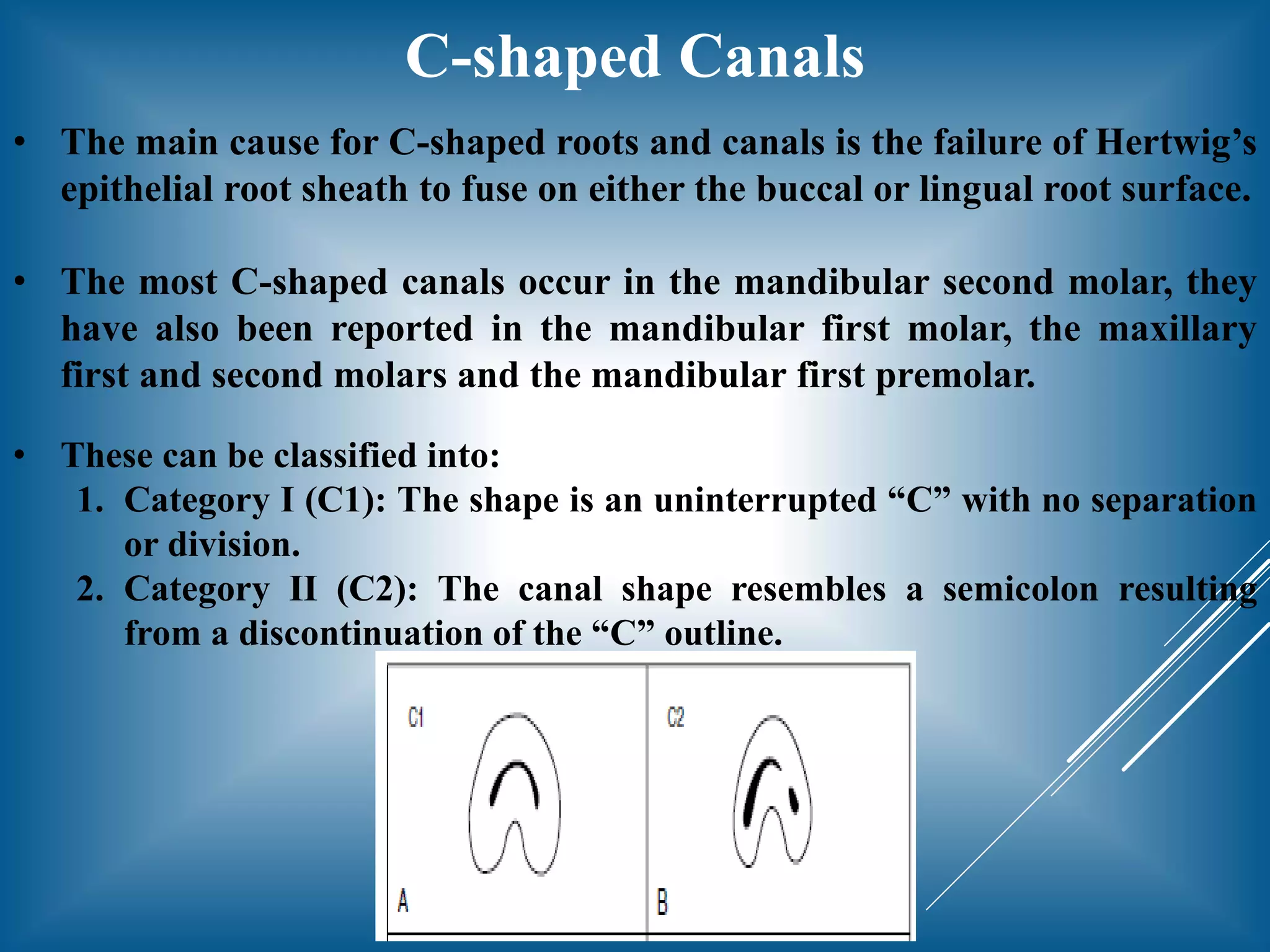
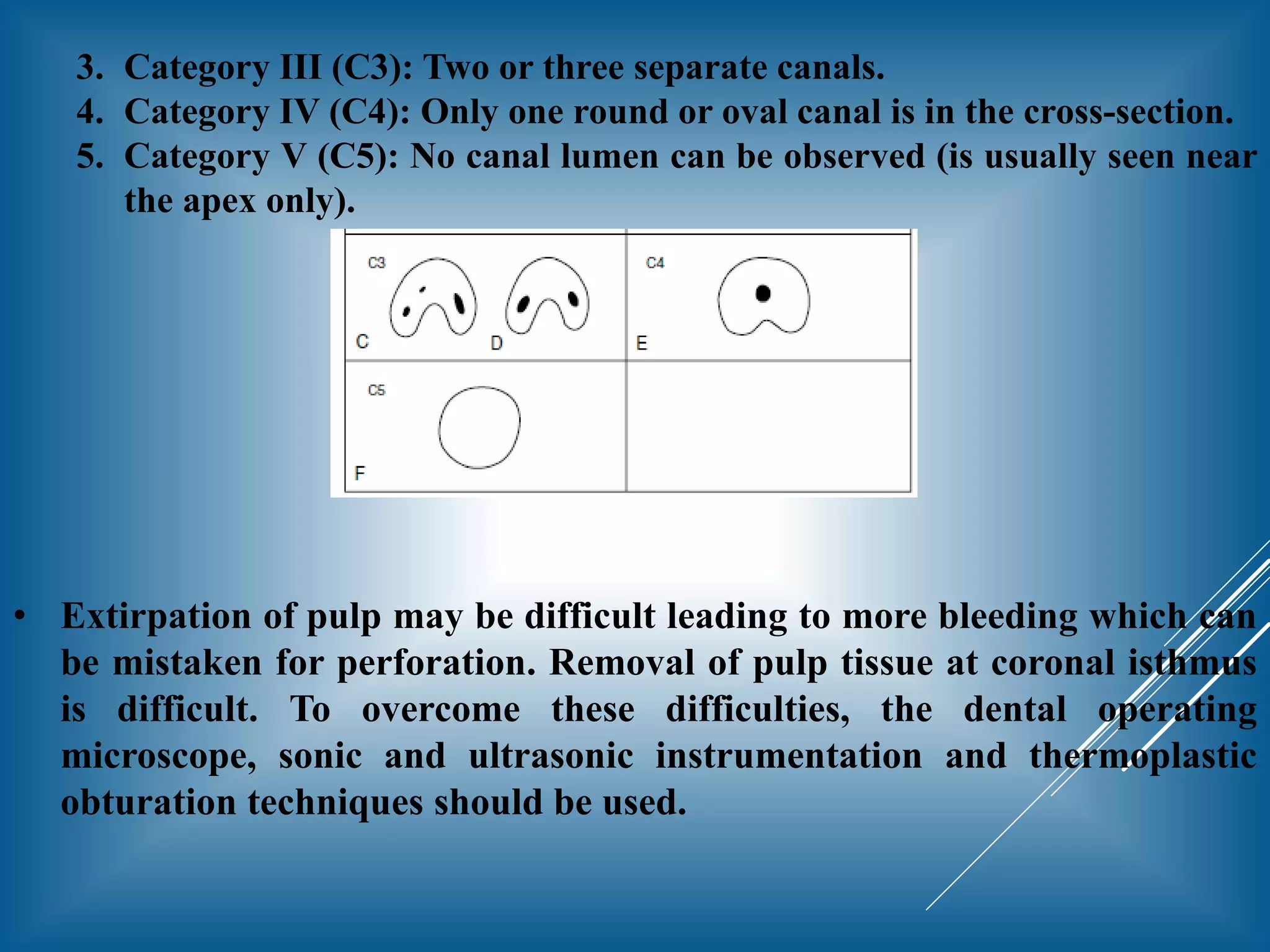

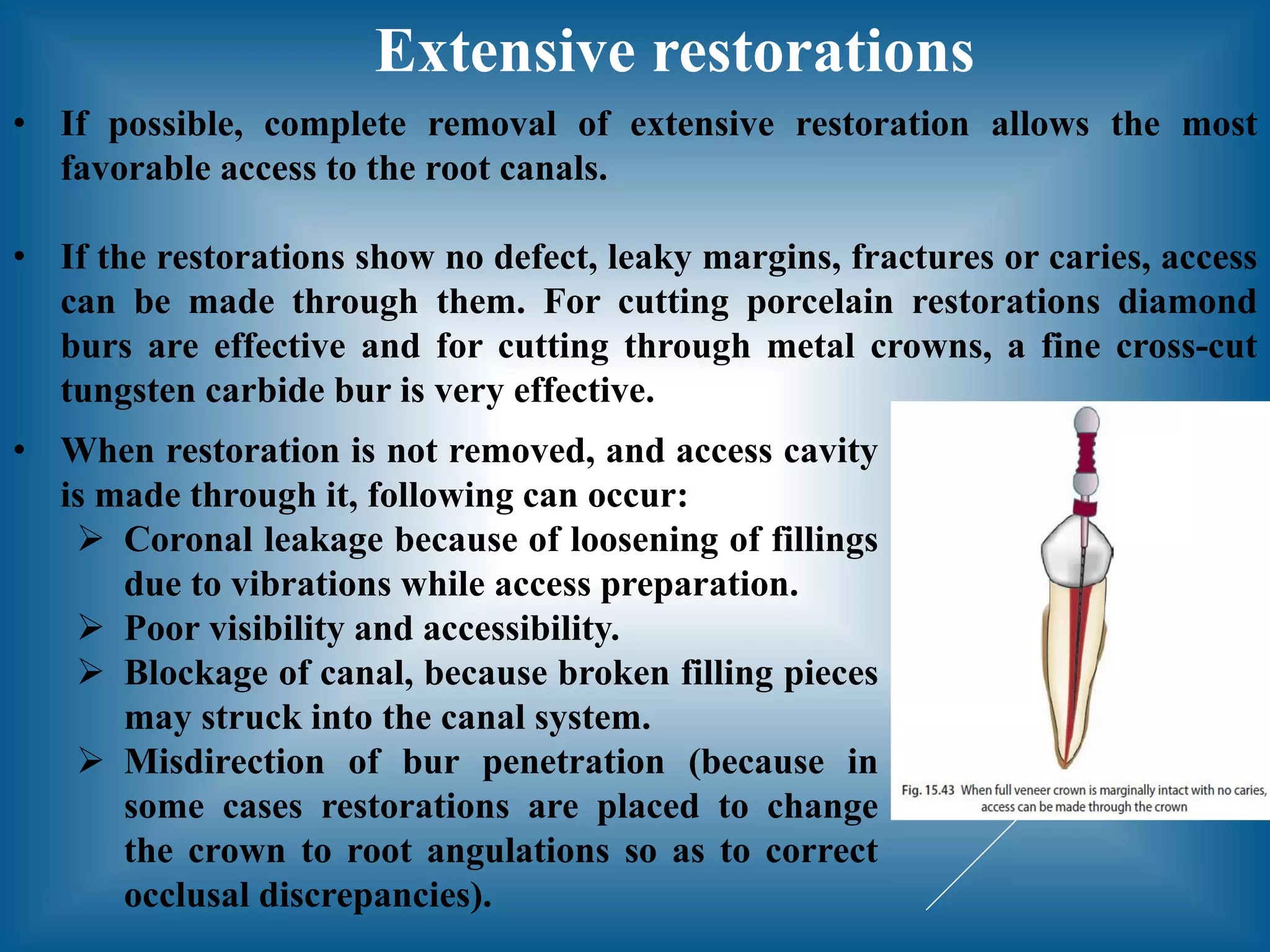
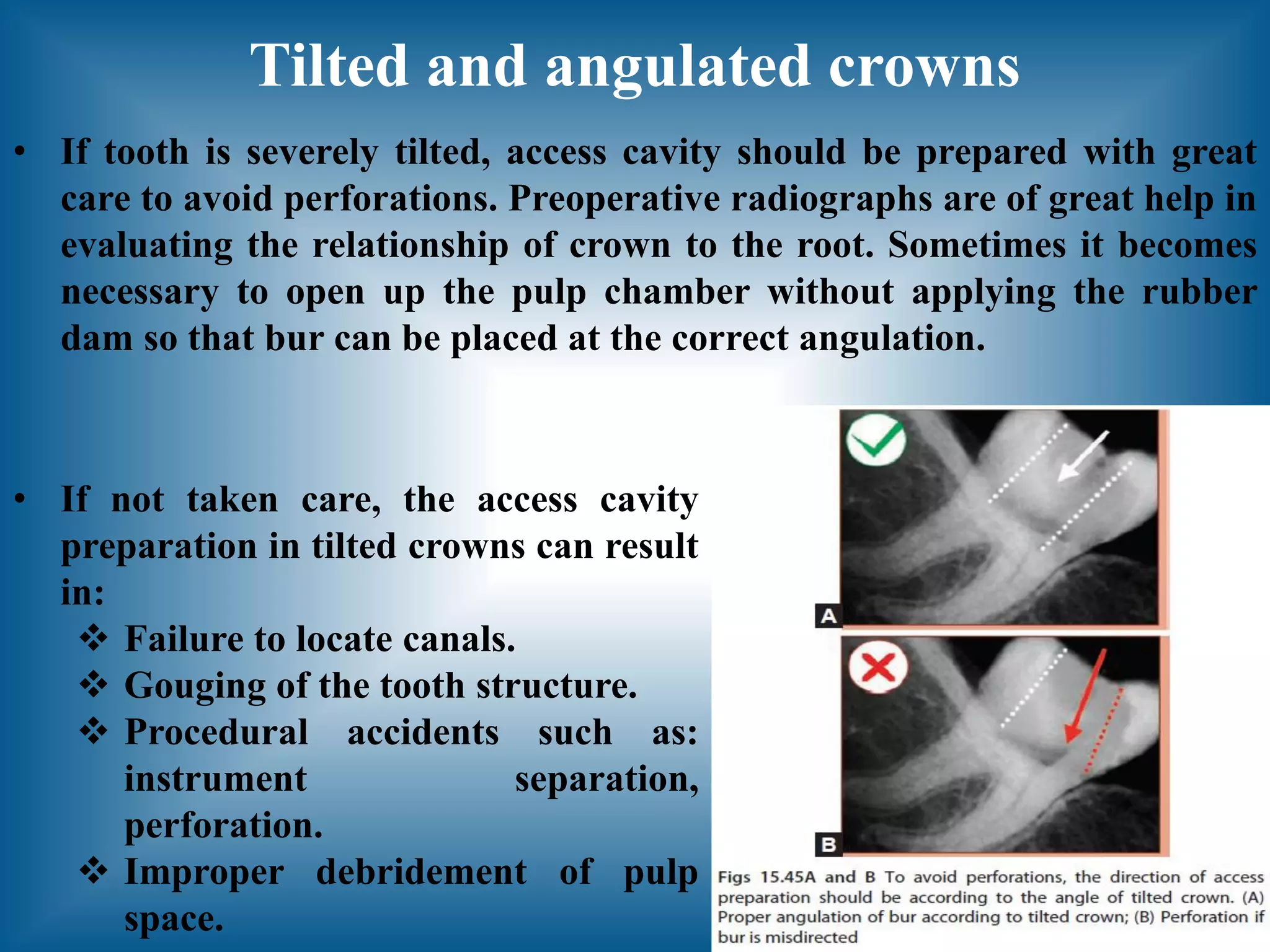

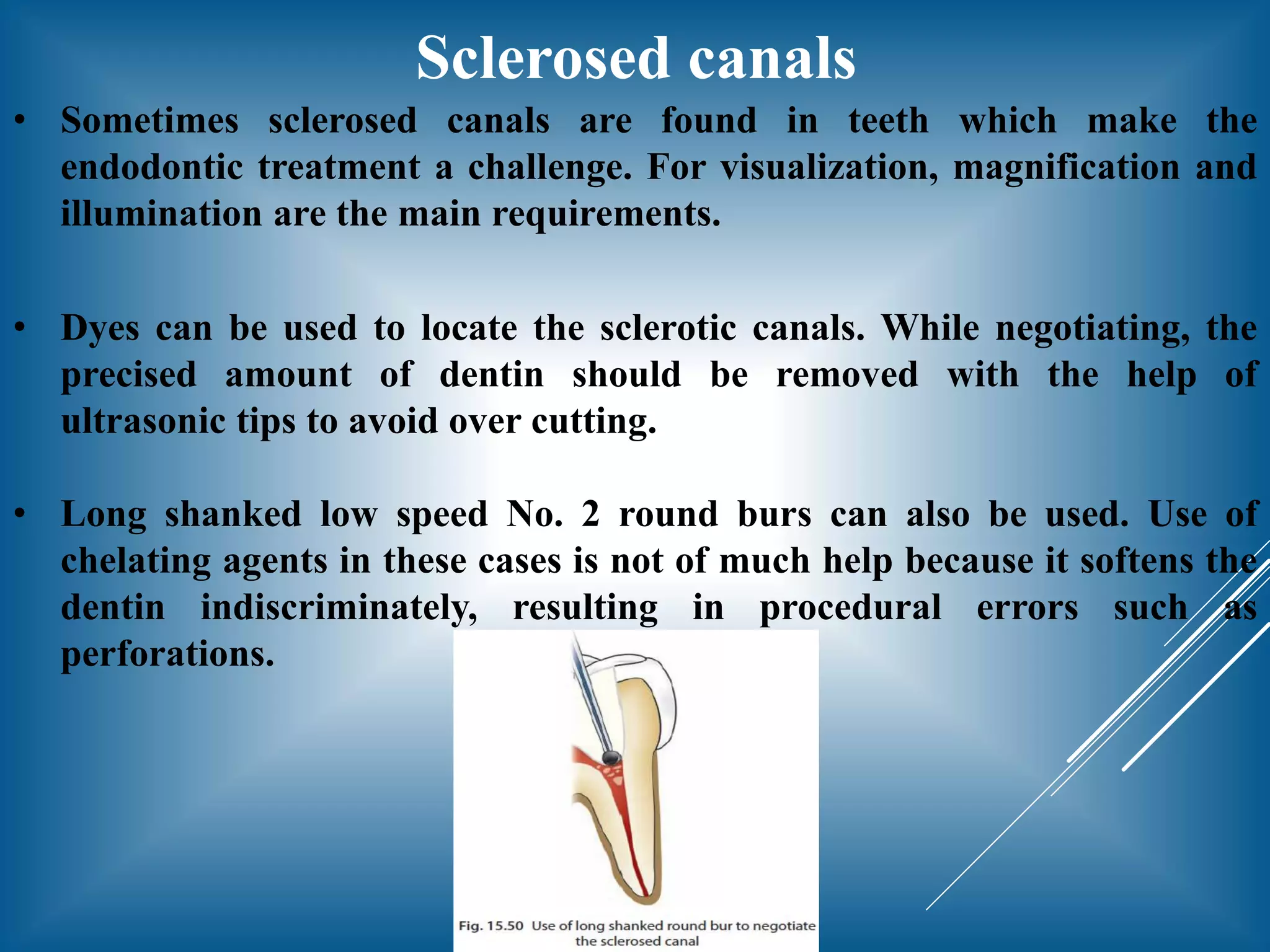


This document discusses principles and guidelines for access cavity preparation in endodontic treatment. It outlines the basic principles established by G.V. Black, including outline form to establish complete access, convenience form to make procedures more convenient, and removal of remaining caries and defective restorations. Guidelines include centrality and concentricity of the pulp chamber floor, using the cementoenamel junction as a landmark, and symmetry of canal orifices. Specific access preparations are described for maxillary and mandibular molars and premolars. Considerations are provided for anatomical variations, extensive restorations, tilted/angled crowns, calcified canals, and teeth with minimal crowns.


























































































