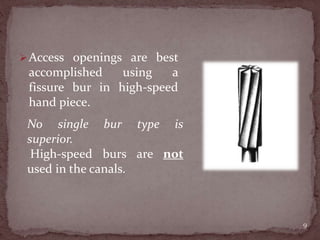
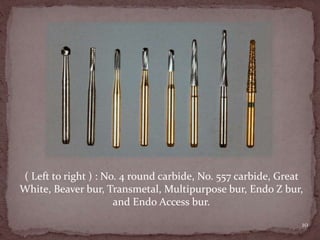
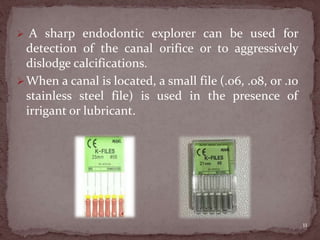
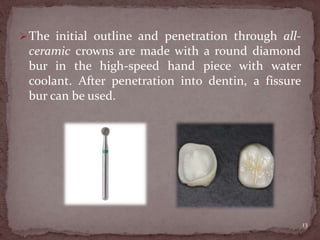
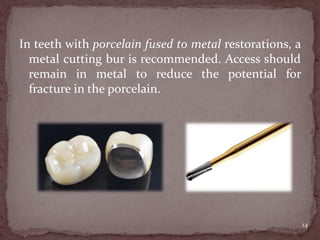
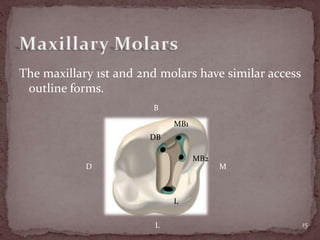
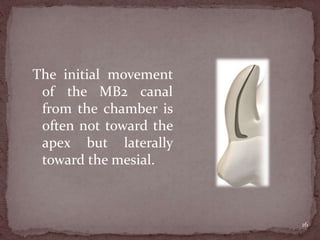
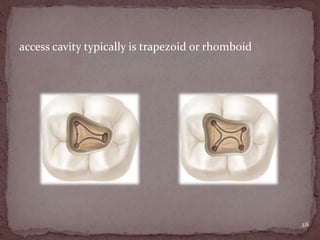
The document discusses the objectives and techniques for preparing access openings for root canal treatment. The major objectives are locating all canals, achieving straight-line access to the canals, removing coronal pulp tissue, and conserving tooth structure. An outline form is recommended for the access shape to correspond to the internal anatomy. Caries must be removed to create an aseptic environment before treatment. Crowns and restorations may need to be removed if they interfere with access. Common access shapes are described for different tooth types. Multiple canal configurations are possible and should be located with small files and irrigation. Inadequate or excessive removal of tooth structure can compromise treatment.