The document provides an overview of abdominal trauma, including its classification, clinical presentation, diagnosis, and management. Some key points:
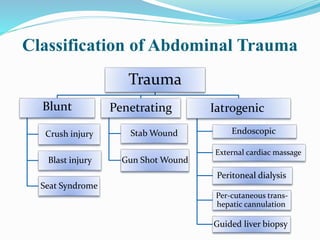
- Abdominal injury is a major contributor to trauma deaths and frequently occurs with multiple injuries, posing management challenges.
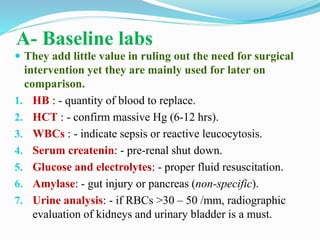
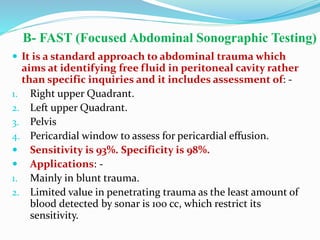
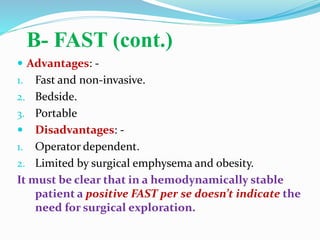
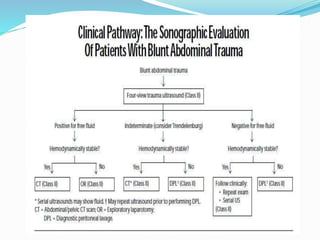
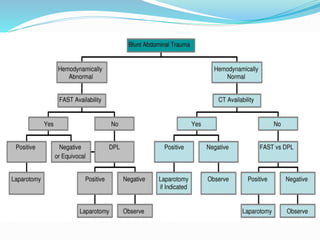
- Diagnosis involves history, physical exam, and directed investigations like FAST ultrasound, CT scan, DPL, and laparoscopy to identify need for surgery.
- Treatment depends on injury type and stability, ranging from non-operative management of solid organ injuries to laparotomy adhering to damage control principles.
- Abdominal compartment syndrome can arise from massive intestinal edema and require decompression techniques like silo bag closure or vacuum pack.










































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















