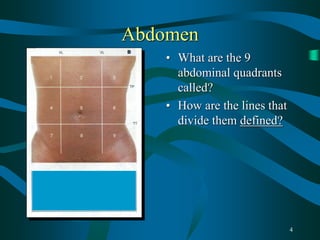
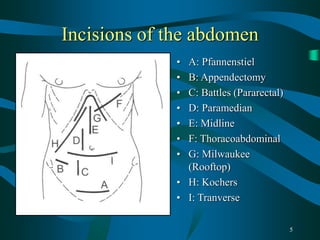
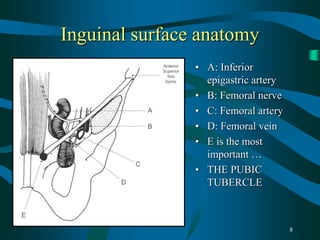
This document provides guidance for final year medical students on examining the abdomen and hernias, investigating scrotal swellings, examining stomas, diagnosing small and large bowel obstructions, evaluating abdominal masses, and disorders of the colorectum and oesophagus/stomach. Key points covered include the nine abdominal quadrants, common incision sites, distinguishing inguinal hernia types, investigating hydroceles, and distinguishing simple from strangulated bowel obstructions. Common colorectal disorders like cancer, diverticulitis, and inflammatory bowel disease are also summarized.