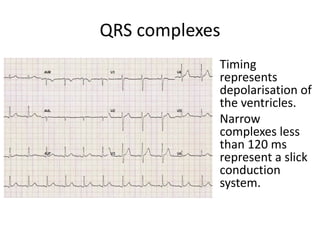
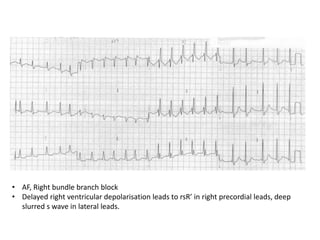
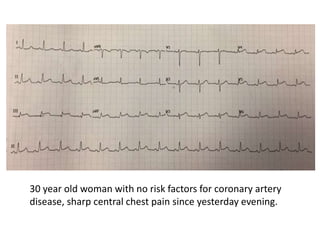
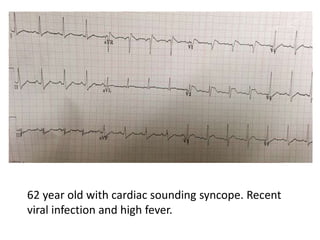
The document details a structured approach to interpreting ECGs, emphasizing the importance of understanding heart rhythms, voltages, and complex timings. It covers technical factors, characteristics of different ECG components, and their clinical implications, such as diagnosing myocardial infarctions. Contextual clinical scenarios highlight the necessity of considering patient history and symptoms when analyzing ECG results.




![ECG & Heart block [doctors online]](https://cdn.slidesharecdn.com/ss_thumbnails/ecgheartblockdoctorsonline-131111054313-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter01.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter01-150421101218-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter15.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter15-150421104606-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter16.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter16-150421104734-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter02.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter02-150421101545-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)










![Shadechapter13.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter13-150421104054-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter09.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter09-150421103043-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




