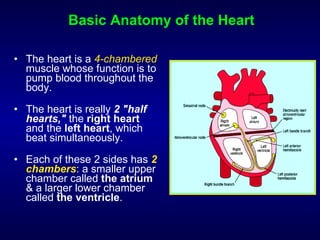
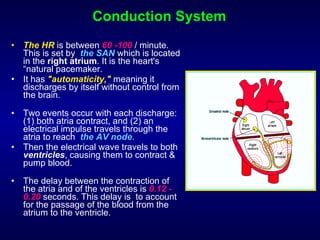


The document provides an overview of electrocardiograms (ECGs), including their purpose, how they work, and what they can reveal about heart conditions. It discusses the basic anatomy and electrical conduction system of the heart. It then explains how ECGs are performed and interpreted, covering the different waves that are measured and what they indicate about heart rate, rhythm, and chambers of the heart. Abnormal findings are also briefly outlined.