Downloaded 14 times
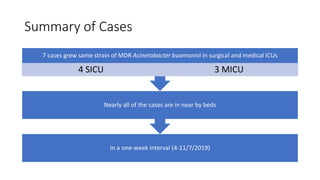
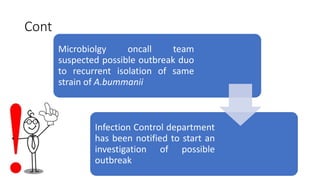
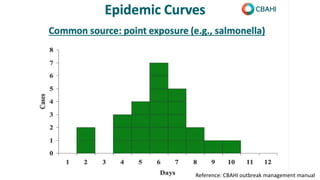
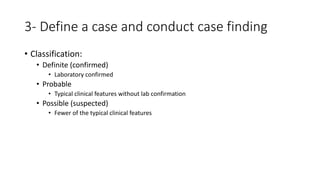
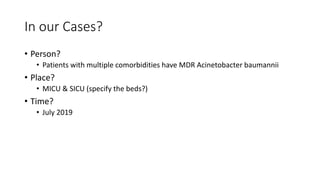
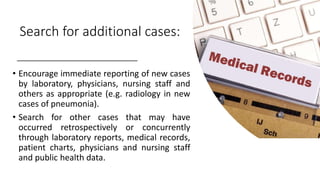
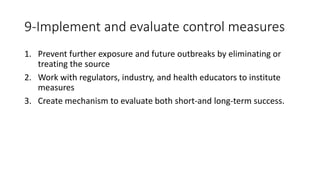



This document outlines the processes for investigating acute infectious disease outbreaks in hospital settings, emphasizing the importance of identifying and eliminating sources of infection to prevent additional cases. It details definitions related to outbreaks, steps for investigation, and case scenarios related to a specific outbreak of multi-drug resistant Acinetobacter baumannii. The document also highlights the role of microbiology labs, criteria for identifying outbreaks, and recommended infection control measures.













































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








