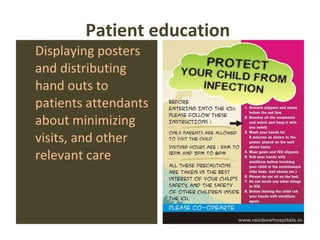
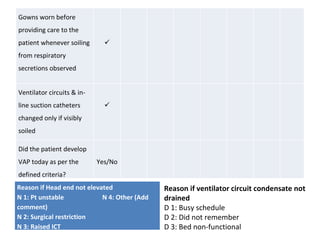


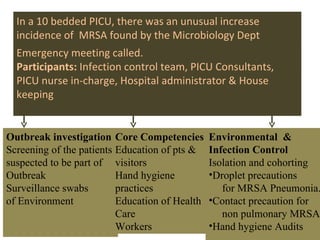


An infection control nurse informed the PICU consultant that two patients have been found to have MDR Acinetobacter infections. This may constitute an Acinetobacter outbreak. The consultant should confirm it is an outbreak by investigating patients and the environment, calculating the attack rate, and comparing it to the background rate. If confirmed, treatment and prevention measures should be implemented, including isolation, cohorting, strict sterilization and disinfection procedures.









































![Employee's' health clinic orientation [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/employeeshealthclinicorientationcompatibilitymode-140123022438-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)













































