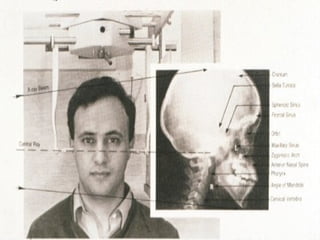
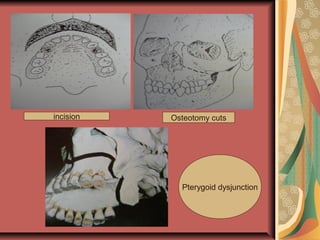
This document discusses various maxillary osteotomies and orthognathic surgery procedures. It describes common maxillary deformities and the evaluation and planning process. Several maxillary osteotomy techniques are outlined, including segmental, total, Le Fort I, II, and III osteotomies. Key steps for each technique like incisions, osteotomy cuts, down fracture, and fixation are summarized. The roles of presurgical orthodontics and postsurgical orthodontics are also briefly discussed.