The document discusses various orthodontic techniques used to gain space for tooth movement, including proximal stripping, expansion, extraction, distalization, molar uprighting, posterior tooth derotation, and anterior tooth proclination. It provides details on when and how to use each technique, their advantages and disadvantages, and diagnostic aids. The goal of these space gaining techniques is to correct malocclusions by moving teeth into more ideal positions.

![[D2-E2-P2-U]
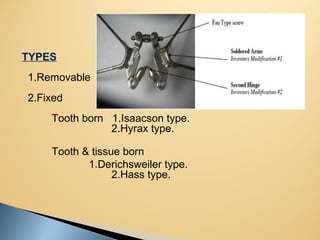
Proximal stripping
Expansion
Extraction
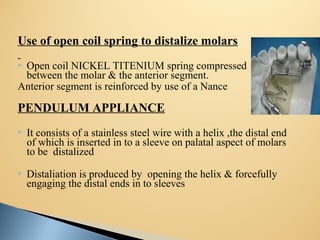
Distalization
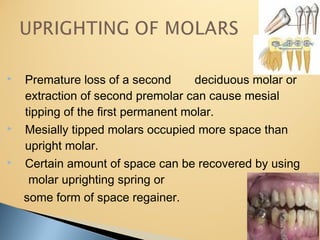
Uprighting of molars
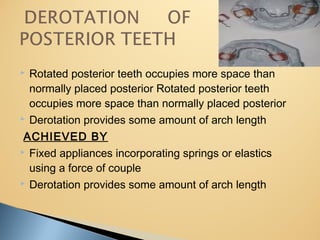
Derotation of posterior teeth
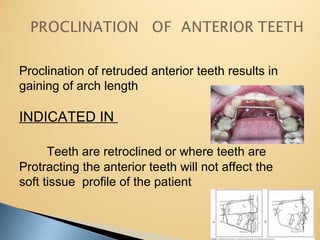
Proclination of anterior teeth](https://image.slidesharecdn.com/methodsofgainingspacefinal-160726165906/85/Methods-of-gaining-space-final-4-320.jpg)










![FACEMASK CHINCUP SEMINAR[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/facemaskchincupseminar1-230916061625-e0964de8-thumbnail.jpg?width=640&height=640&fit=bounds)










































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)













