Downloaded 35 times









1. The document discusses treatment options for skeletal malocclusions, including growth modification, orthodontic camouflage, and orthognathic surgery. 2. Pre-surgical orthodontic treatment aims to prepare the patient for surgery through procedures like alignment, decompensation, and creating space for osteotomies. 3. Surgical procedures discussed include Le Fort I osteotomy for the maxilla, bilateral sagittal split osteotomy for the mandible, and genioplasty for the chin. Post-surgical orthodontics establishes the final occlusion.









































































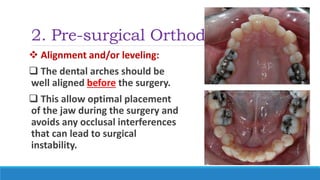
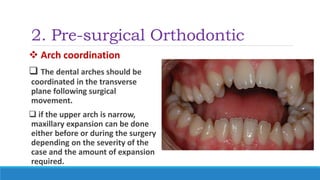
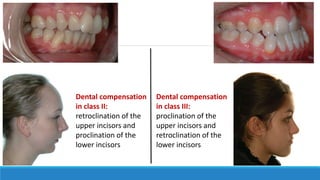
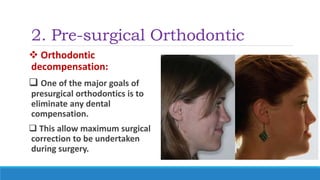
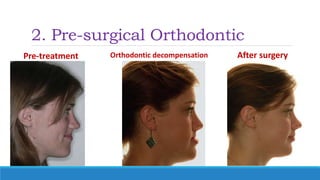
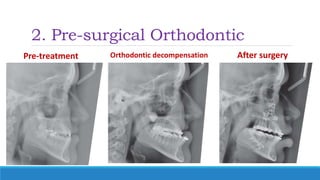
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













