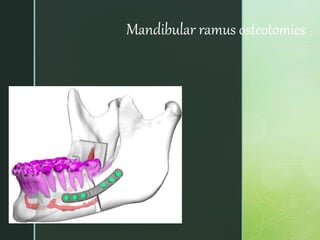
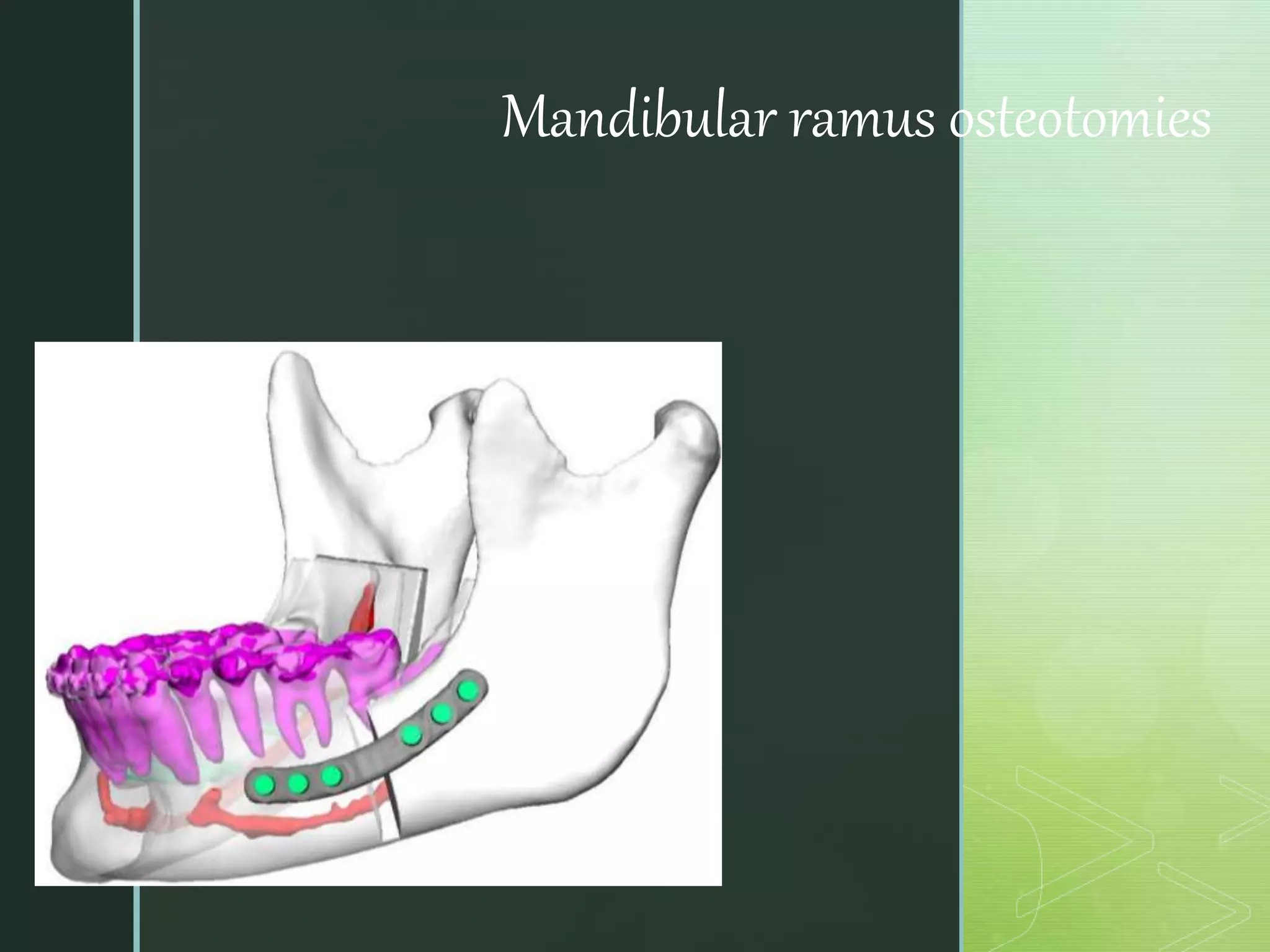
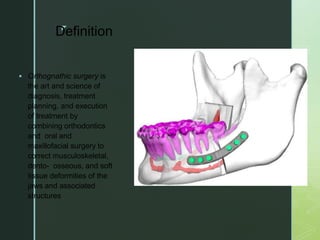
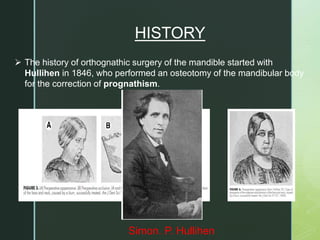
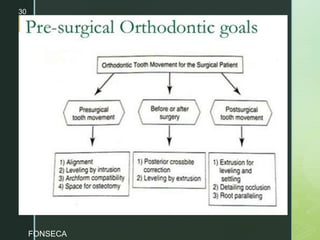
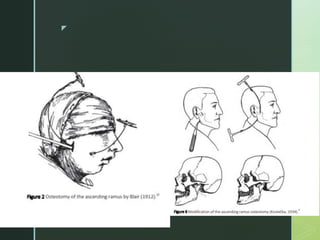
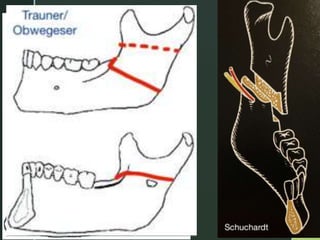
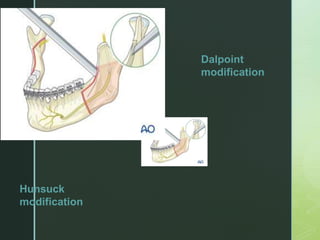
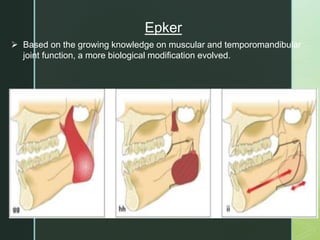
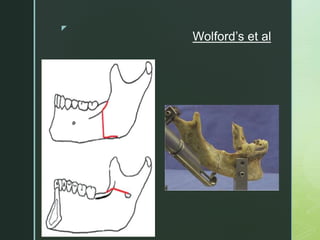
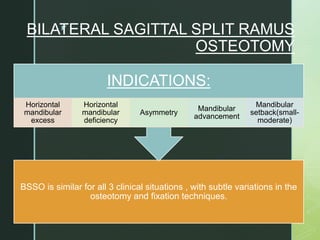
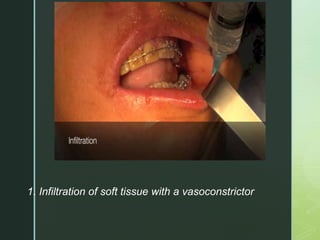
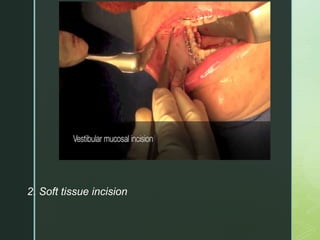
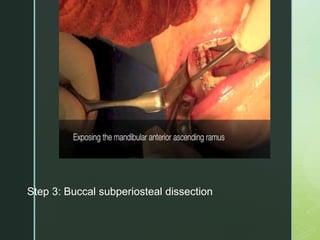
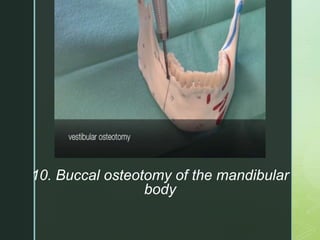
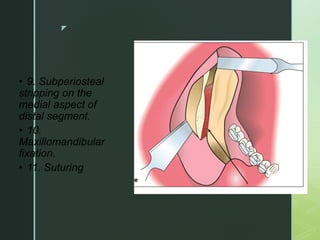
Mandibular ramus osteotomies are performed as part of orthognathic surgery to correct jaw deformities. The history began in the 1840s with body osteotomies and evolved to include ramal osteotomies from the 1920s-1940s. The bilateral sagittal split ramus osteotomy (BSSO) technique described in the 1950s-60s became the standard for mandibular setbacks and advancements. BSSO involves segmental osteotomies, splitting the mandible, repositioning segments, and fixation with plates or screws. Alternative techniques like vertical ramus osteotomy preserve the inferior alveolar nerve but limit distal segment movement. Careful preoperative









































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
