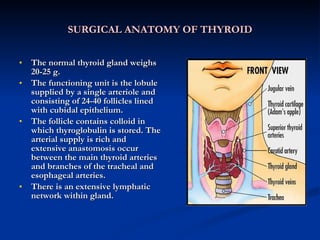
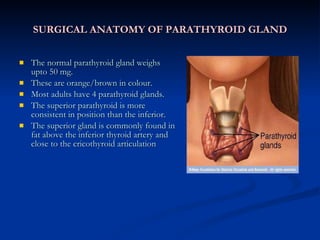
The document discusses the embryology, anatomy, physiology and diseases of the thyroid and parathyroid glands. It describes how the thyroid develops from the pharynx and how the parathyroid glands develop from pouches in the pharynx. It discusses the location and function of the thyroid and parathyroid glands, and how thyroid hormones are synthesized and regulated. It also summarizes the causes, symptoms, diagnosis and treatment of hypothyroidism.