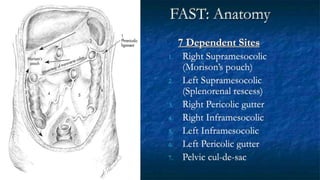
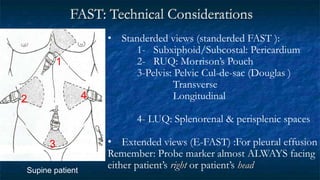
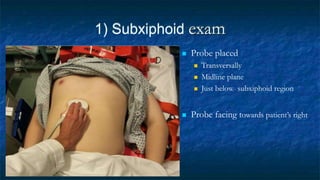
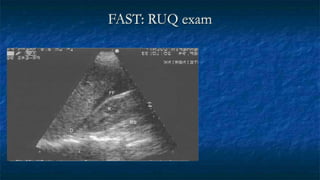
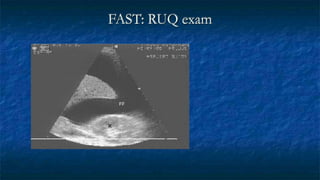
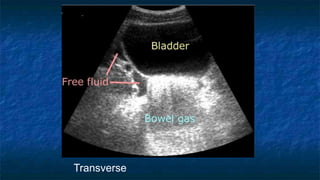
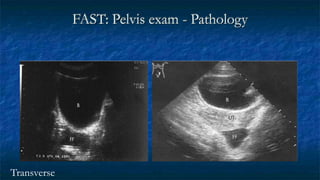
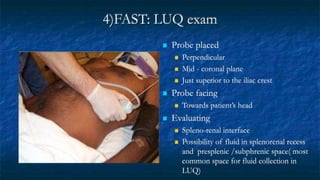
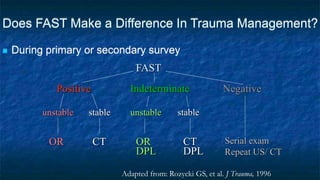
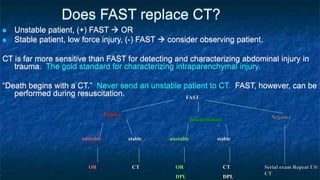
FAST (Focused Assessment with Sonography in Trauma) is an ultrasound technique used to quickly detect the presence of free fluid in the abdomen or chest resulting from trauma. It can visualize fluid in seven dependent areas of the abdomen and the pericardial sac. FAST has sensitivity of 88-91.7% and specificity of 94.7-99% for detecting fluid. A positive FAST means fluid is detected in one of the areas scanned, while a negative FAST means no fluid is seen. FAST provides a rapid initial assessment and can help guide trauma management, but CT is more sensitive for characterizing injuries. Limitations include difficulty with obese patients, bowel gas, or retroperitoneal injuries.