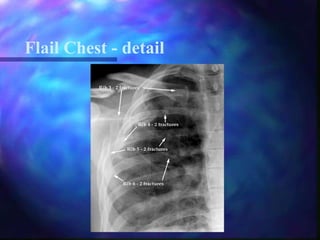
Chest trauma can be life-threatening and accounts for 25% of all trauma deaths. It includes injuries from blunt forces like rib fractures or penetrating injuries from stab wounds. Without treatment, injuries can lead to hypoxia and hypotension from issues like pneumothorax, hemothorax, or flail chest. Proper management requires following ABC (airway, breathing, circulation) to ensure oxygen delivery and addressing specific injuries like tension pneumothorax through needle decompression or chest tube insertion.