This document discusses shock in trauma and provides an overview of key topics including:
- The pathophysiology of shock involves inadequate oxygen delivery leading to cellular dysfunction.
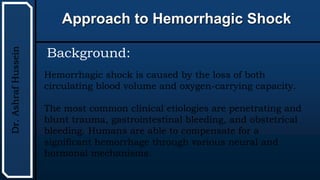
- Hypovolemic shock from blood or fluid loss is a leading cause and requires rapid fluid resuscitation.
- A thorough physical exam and diagnostic tests are needed to identify the source of bleeding.
- Early intervention and resuscitation are important to reverse the effects of shock and reduce mortality.


















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















