Downloaded 37 times
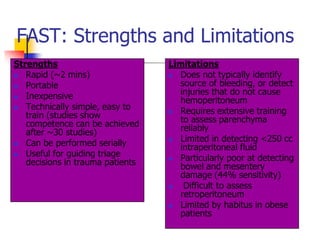
![Objective
To determine the accuracy of emergency
nurses in detecting free fluid in abdomen
when compared to radiologist during primary
survey of trauma victims by focused
assessment with Sonography for trauma
[FAST] scan in the Emergency Department
[ED].](https://image.slidesharecdn.com/fastbynursesppt-111228222943-phpapp01/85/Fast-by-nurses-ppt-3-320.jpg)
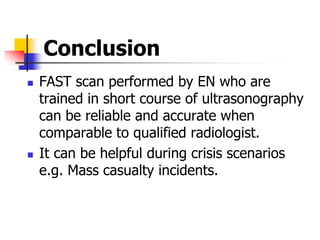
![Results
94 scans performed each by EN and RR were
analysed.
Mean age of the patients was 29 [2 - 85] years.
Out of 23 true positive patients 18 underwent CT
scan and exploratory laparotomy was done in 14
patients.
Sensitivity of FAST done by EN and RR was 90 %.
Specificity of FAST done by EN was 94.6 %Vs RR.
Positive predictive value and negative predictive
values were 81.8% and 97.2% respectively](https://image.slidesharecdn.com/fastbynursesppt-111228222943-phpapp01/85/Fast-by-nurses-ppt-12-320.jpg)


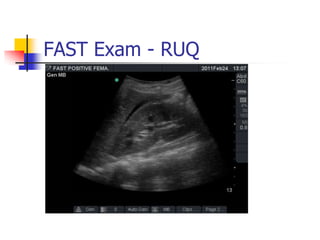
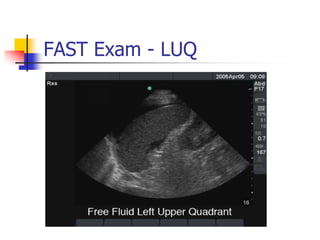
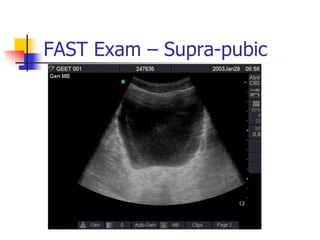
Emergency nurses who underwent training in focused assessment with sonography for trauma (FAST) scanning showed comparable accuracy to radiologists in identifying free fluid in trauma patients, with a sensitivity of 90% for both groups. While FAST scanning provides a rapid, portable, and inexpensive option for initial trauma evaluation, it does not identify the source of bleeding and has limitations in detecting certain injuries.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)