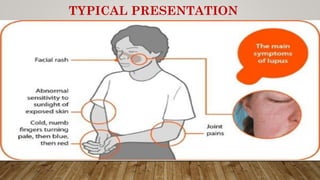
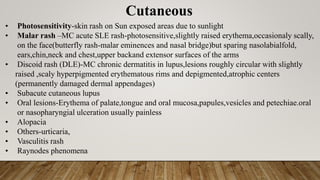
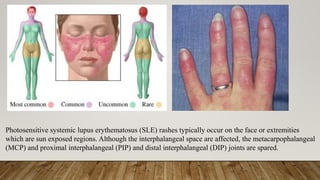
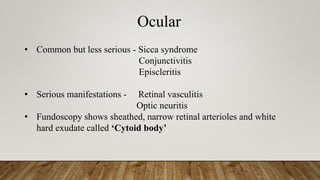
Systemic lupus erythematosus (SLE) is an autoimmune disease that can affect multiple organ systems. Key signs and symptoms include malar rash, arthritis, oral ulcers, photosensitivity, serositis, renal disease, and hematological abnormalities. Diagnosis involves evaluating clinical criteria along with identifying autoantibodies. Treatment aims to induce remission during flares using glucocorticoids and immunosuppressants to prevent organ damage.

![Systemic+ Lupus+ Erythematosus
Systemic - The disease can affect organs and tissues throughout the
body.
Lupus [ Latin for wolf ] It refers to the rash that was thought to
resemble a wolf bite.
Erythematosus [ Greek word for red ] – It refers to the color of the
rash.](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-2-320.jpg)


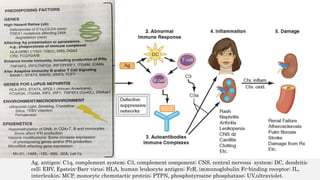
![Role of Genetics and Environment
➢Environment
• Cell damage by environmental triggers causes apoptosis that leads to release of
apoptotic bodies+parts of nucleus [ now exposed to other parts of body ]
➢ Genetics – Susceptibility genes and their effect on immune system.
• loss of self tolerance [ immune system recognizes parts of nucleus as self antigens ]
• Self Ag presentation by DCs,
• Defective complement system,
• Impaired clearance of apoptotic cells
• Aberrant lymphocyte activity[unregulated T cell dependent B cell activation]
• Production of autoantibodies](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-13-320.jpg)
![• Antigen-Antibody complexes / Immune Complexes deposition in various body tissues
[ basement membranes ] results
– Local inflammation
– Local complement activation
– Local apoptosis
– Positive feedback loop
• DNA is the main antigen for which antibodies are formed
• IgG is the most “pathogenic” because it forms intermediate sized complexes that can get
to the small places and block them
• Injury is caused by
Mainly deposition of immune complexes and
Binding of antibodies to various cells and tissues.
• In most patients, autoantibodies are present for a few years before the first clinical
symptom appears](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-14-320.jpg)

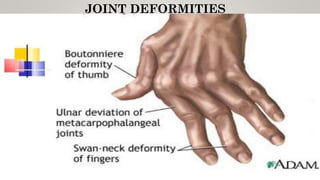
![Musculoskeletal
• Arthralgia , myalgia
• Polyarthritis [ 2 or more peripheral joint ] - Intermittent,mild to disabling,soft tissue swelling,
tenderness,Nonerosive,MC in hands,wrists and knees
• Joint deformities (hands and feet)-In 10% cases ,erosions can be identified on ultrasound
(rarely on x-rays)
• Myopathy /myositis
• Ischemic necrosis of bone
“rhupus”-some patients of SLE have rheumatoid like arthritis with erosions and fulfill
criteria for both RA and SLE so may be coded having both diseases](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-19-320.jpg)
![Thromboembolic events
Patients of Antiphospholipid syndrome due to hypercoagulable state
more prone to clots [ venous or arterial ] that can leads to
• Deep vein thrombosis
• Hepatic vein thrombosis
• Stroke
• Myocardial infarction](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-32-320.jpg)
![LABORATORY TESTS
• Antinuclear antibodies [ANA]-Sensitive but not specific
• Anti -ds DNA-[ More specific ], targets double-stranded DNA, seen during active disease
• 4 RNA associated antibodies -
Anti-Sm [Smith] –[ More specific ]Targets ribonucleoproteins
Anti Ro /SSA- antibody
Anti La/SSB- antibody
Anti –RNP
• Antiphopholipid antibody- [Less specific to Lupus] Targets protein bound to phospholipid
Lupus anticoagulent [ Lupus antibody ]
Anti-B2 glycoprotein 1 AB
Anti-cardiolipin](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-43-320.jpg)
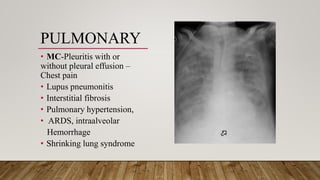
![• Complement levels [ C3 and C4 ] - Decreased (C3 level < 5.5 mg/dl)
• Chest radiography and chest CT scanning-
ILD, pneumonitis, pulmonary emboli, alveolar haemorrhages
• Joint radiograpy-periarticular osteopenia and soft tissue swelling without
erosions
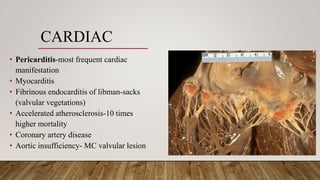
• Echocardiography-pericardial effusion
• ↑ ESR, ↑ anti ds-DNA and ↓C3 may indicate disease ‘flare’](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-45-320.jpg)

![Conservative management
• NSAIDs, salicylates (Ecotrin a and St. Joseph’s aspirin approved by FDA for use in SLE )
for arthritis / arthralgia- Doses toward upper limit of recommended range usually required
• Antimalarials(HCQ,CQ,quinacrine)-for dermatitis, arthritis, fatigue
• Systemic glucocorticosteroids( low dose)
• Belimumab
• lupus dermatitis-topical sunscreens [ SPF 15 at least ; 30+ preferred],antimalarials, topical
glucocorticoids and/or tacrolimus and systemic glucocorticoids with or without
mycophenolate for severe or unresponsive cases](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-52-320.jpg)
![Cytotoxic/immunosuppressive therapy
➢ Methotrexate
[for dermatitis, arthritis]
10–25 mg once a week, PO or SC, with folic acid; decrease dose if CrCl<60 mL/min
➢ Cyclophosphamide
• IV
Low dose : 500 mg every 2 weeks for 6 doses maintenance with MMF or
AZA. High dose: 7–25 mg/kg q month × 6; consider mesna administration
with dose
• Oral
1.5–3 mg/kg per day; decrease dose for CrCl <25 mL/min](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-55-320.jpg)
![• Mycophenolate
MMF: 2–3 g/d PO for induction therapy,
1–2 g/d for maintenance therapy; max 1 g bid if CrCl <25 mL/min
MPA: 360–1080 mg bid; caution if CrCl<25 mL/min
• Azathioprine
2–3 mg/kg per day PO for induction; 1–2 mg/kg per day for maintenance; decrease frequency
of dose if CrCl <50 mL/min
• Belimumab
10 mg/kg IV wks 0, 2, and 4, then monthly
• Rituximab
[ for patients resistant to above therapies ]
375 mg/m2 q wk × 4 or 1 g q 2 wks × 2](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-56-320.jpg)
![Lifestyle changes to help cope with SLE.
• Get plenty of rest (fatigue is another common SLE symptom)
• Salt restriction [ if HTN ] , avoid fat [ for hyperlipidaemia ] , calcium supplements with
steroid therapy
• Engage in regular light-to-moderate exercise to help fight fatigue and heart disease, and to keep
joints flexible
• Avoid excessive sunlight exposure, and wear sunscreen (ultraviolet light is the one of the main
triggers of flares)
• Don't smoke and avoid exposure to second-hand tobacco smoke](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-59-320.jpg)
![PREVENTIVE THERAPIES
Prevention of complications of SLE and its therapy
• Suppressing recurrent urinary tract infections.
• Providing appropriate vaccinations [ the administration of influenza and pneumococcal ]. [
Vaccination with attenuated live viruses is generally discouraged in patients who are
immunosuppressed ].
• Prevention of osteoporosis .
[ Postmenopausal women can be protected from steroid-induced osteoporosis
with either bisphosphonates or denosumab. Safety of long-term use of these
strategies in women is not well established ].
• Control of hypertension
• Prevention strategies for atherosclerosis
monitoring and treatment of dyslipidemias
management of hyperglycemia and obesity.](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-60-320.jpg)
![Pregnancy and Lupus
• Fertility rates for men and women with SLE are probably normal.
• Rate of fetal loss is increased (approximately two- to threefold) in women with SLE.
• Fetal demise is higher in mothers with high disease activity, antiphospholipid antibodies,
and/or active nephritis.
• Suppression of disease activity can be achieved by administration of systemic
glucocorticoids.
• Glucocorticoids [ Pregnancy category A (no evidence of teratogenicity in human studies)]
• Cyclosporine, tacrolimus, and rituximab [category C (may be teratogenic in animals but no
good evidence in humans) ];
• Azathioprine, hydroxychloroquine, mycophenolate mofetil, and cyclophosphamide
[category D (there is evidence of teratogenicity in humans, but benefits might outweigh
risks in certain situations) ];
• Methotrexate [ category X (risks outweigh benefits)].](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-65-320.jpg)
![Lupus Dermatitis
• Minimize exposure to ultraviolet light [ appropriate clothing and sunscreens ] .
• Topical glucocorticoids and antimalarials (such as hydroxychloroquine) reduces lesion
severity in most patients and are relatively safe.
• Systemic treatment with retinoic acid is a useful strategy in patients with inadequate
improvement on topical glucocorticoids and antimalarials; adverse effects are potentially
severe (particularly fetal abnormalities),
• Extensive, pruritic, bullous, or ulcerating dermatitis usually improve promptly after
institution of systemic glucocorticoids; tapering may be accompanied by flare of lesions, thus
necessitating use of a second medication such as hydroxychloroquine, retinoids, or cytotoxic
medications such as methotrexate, azathioprine, or mycophenolate mofetil.
• Topical tacrolimus - In therapy-resistant lupus dermatitis [possible increased risk for
malignancies ] dapsone or thalidomide [ the extreme danger of fetal deformities ]](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-70-320.jpg)
![Poor prognosis (~50% mortality in 10 years) in most series is associated with (at the
time of diagnosis)-
• High serum creatinine levels (>124 μmol/L [>1.4 mg/dL]),
• Hypertension,
• Nephrotic syndrome (24-h urine protein excretion >2.6 g),
• Anemia (hemoglobin <124 g/L [<12.4 g/dL]),
• Hypoalbuminemia,
• Hypocomplementemia,
• Antiphospholipid antibodies,
• Male sex,
• Ethnicity (African American, Hispanic with mestizo heritage) and low socioeconomic
status.
Overall patient survival in SLE patients with renal transplants rejection compared to patients
with other causes of ESRD, is comparable (85% at 2 years).
Lupus nephritis occurs in approximately 10% of transplanted kidneys.](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-75-320.jpg)
![Morbidity-
• Disease associated[ primarily to chronic fatigue, arthritis, and
pain, as well as renal disease ]
• Corticosteroid associated
Mortality-
• Early[in first decade]-Active disease,renal failure and infection
• Late- Atherosclerosis [ thromboembolic events ]](https://image.slidesharecdn.com/diagnosisandmanagementsle-181218123611/85/Diagnosis-and-management-sle-76-320.jpg)

























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)