Download as PDF, PPTX











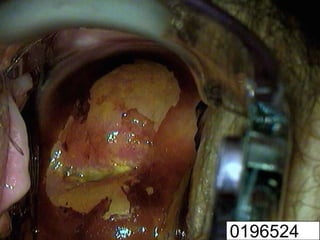




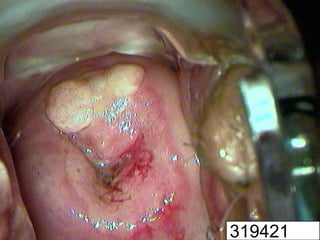
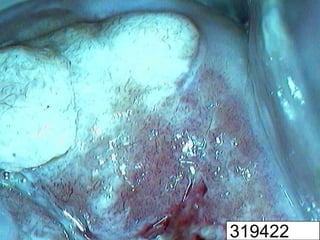






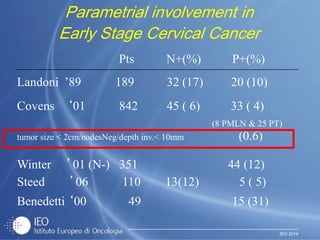
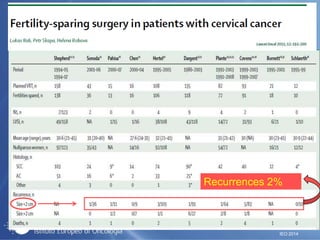
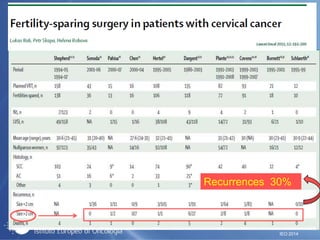
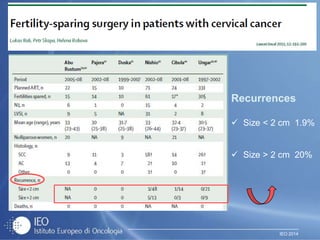
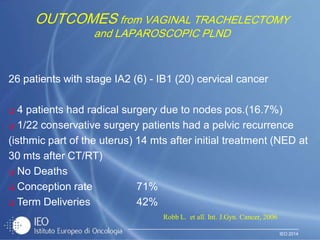



This document discusses treatment approaches for early stage cervical cancer. It notes that for invasive cervical cancers measuring less than 2 cm, removal of the parametrium may be omitted. For some very small tumors, pelvic lymphadenectomy can also be omitted as the risk of lymph node metastasis is limited. It also discusses outcomes from vaginal trachelectomy and laparoscopic pelvic lymphadenectomy for early stage cancers. The document considers conservative treatment approaches for stage IA2-IB1 cancers less than 3 cm in size, including a proposed study design stratifying patients based on tumor diameter.






















































![Management Of Early Stage Ca Cervix [Autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/management-of-early-stage-ca-cervix-autosaved-1233338415127954-2-thumbnail.jpg?width=640&height=640&fit=bounds)