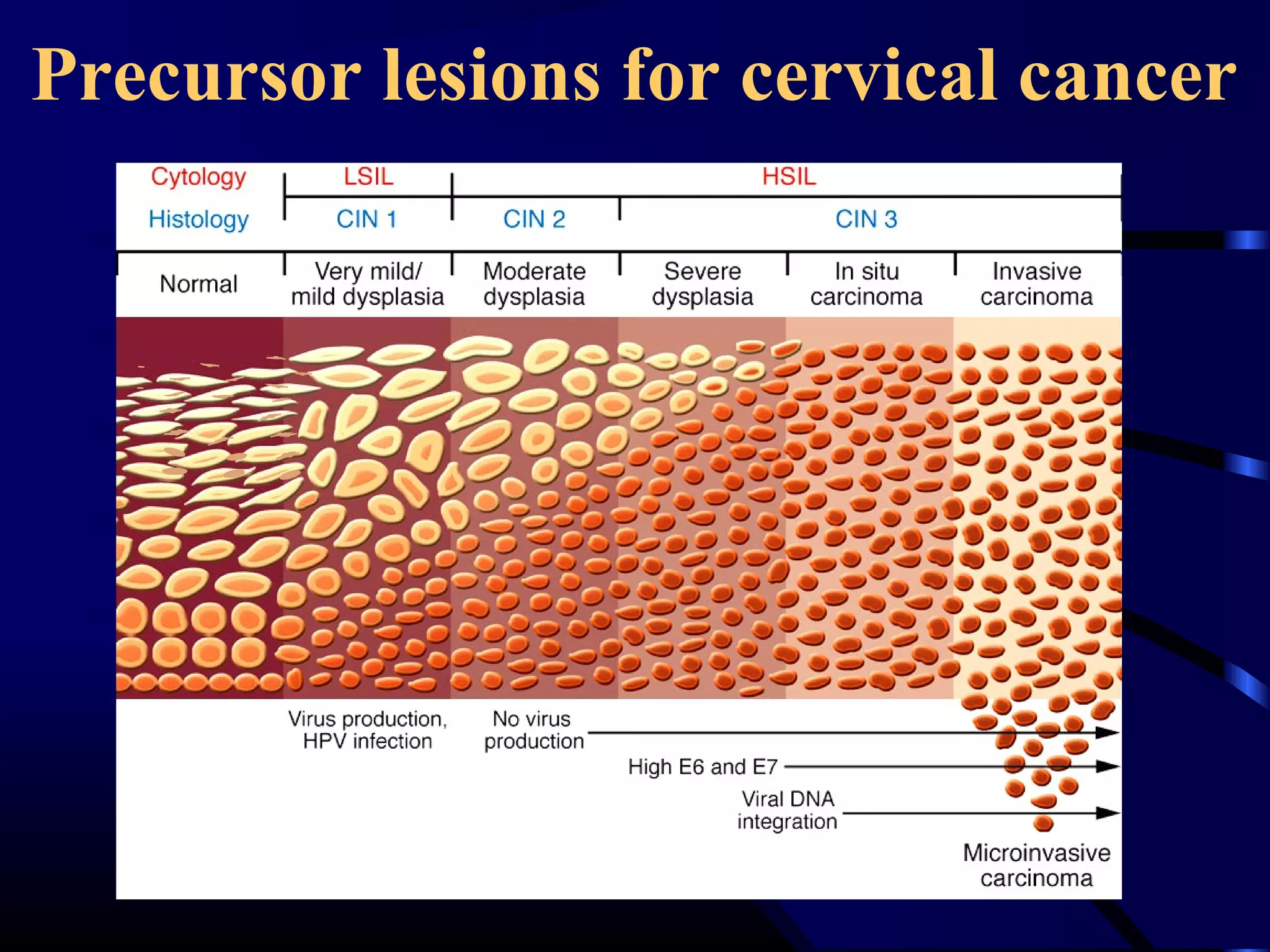
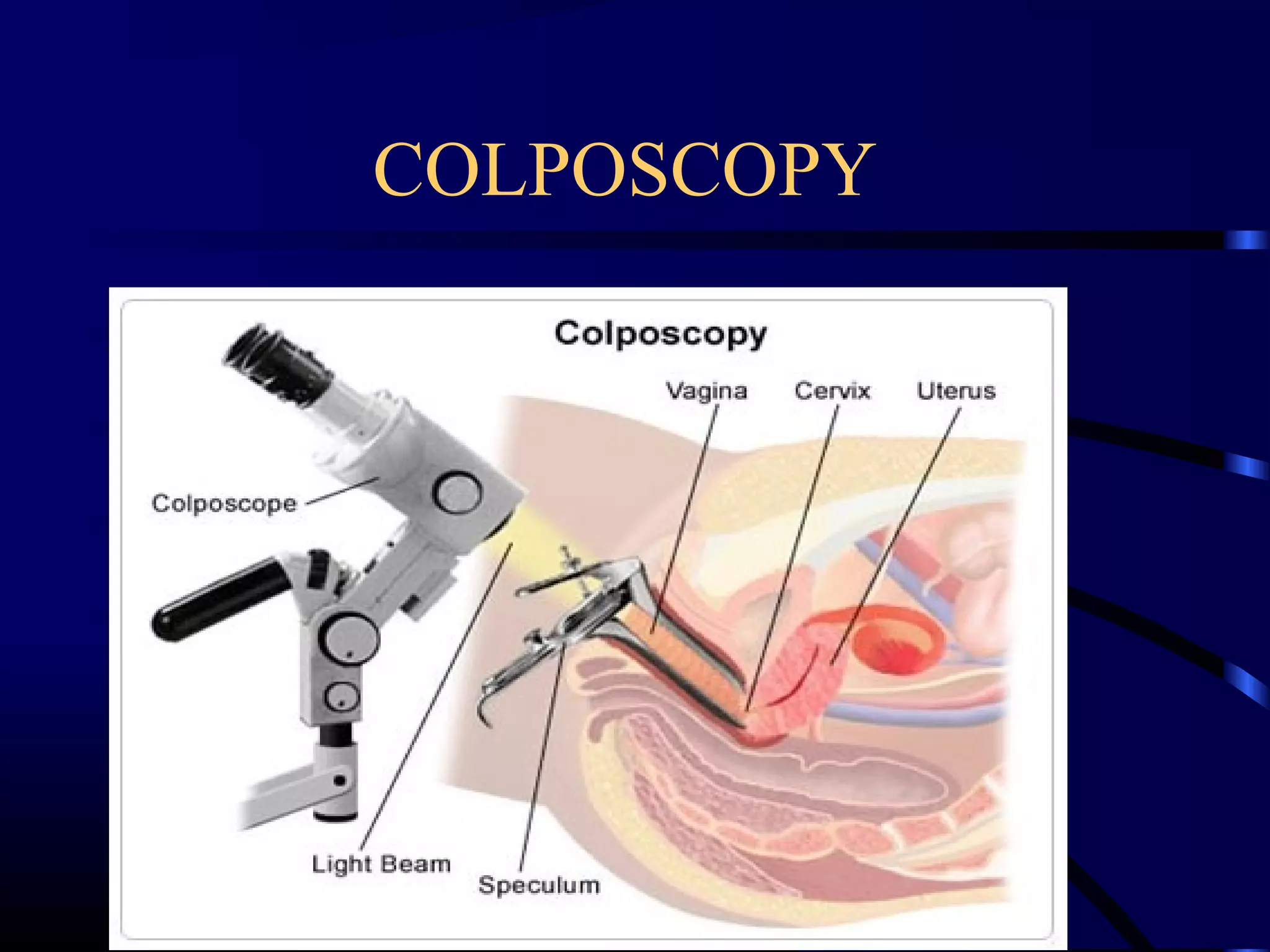
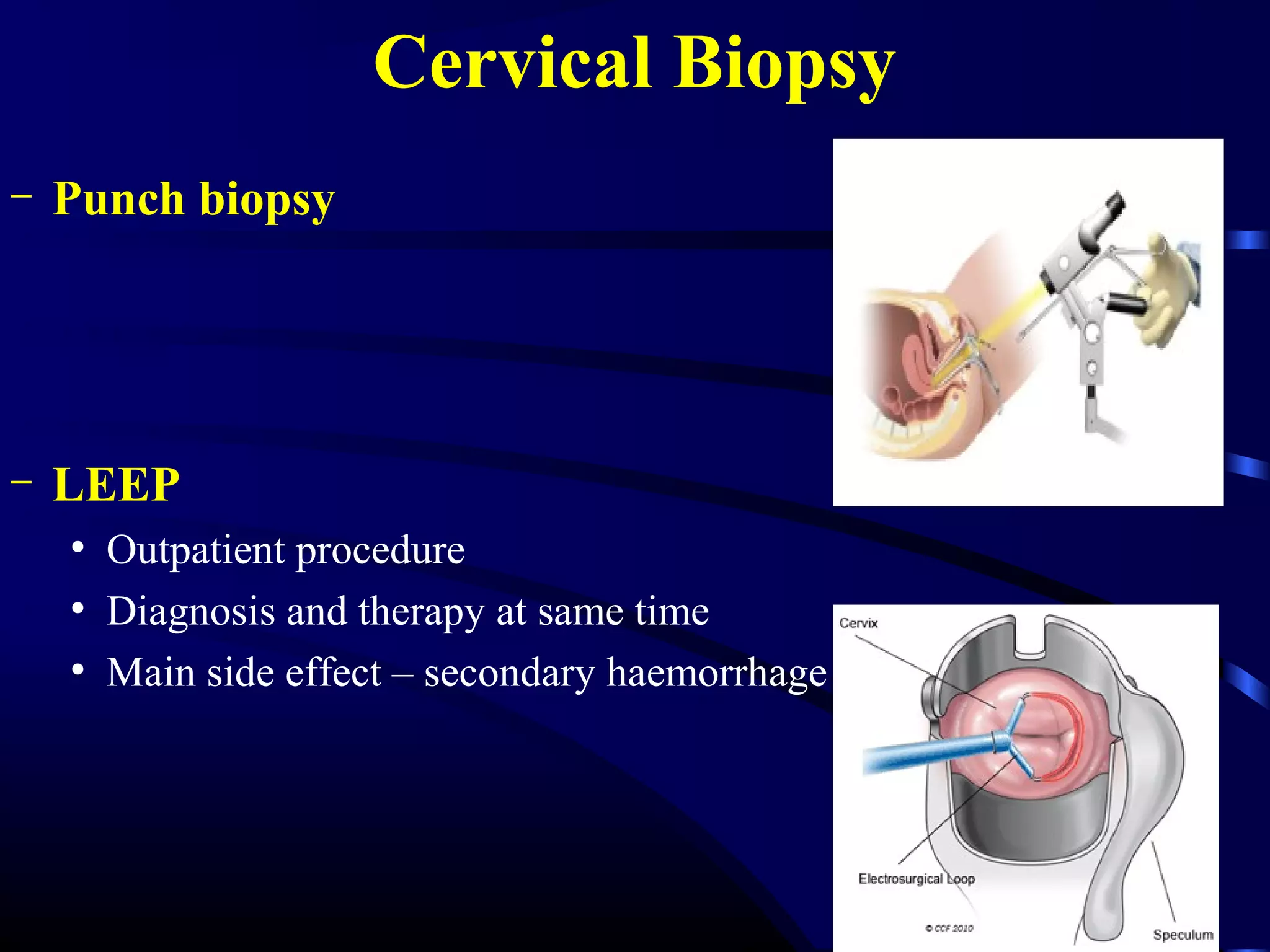
This document discusses cervical cancer, including its causes, diagnosis, staging, and treatment. It begins with the histology and embryological development of the cervix. Precancerous lesions called cervical intraepithelial neoplasia can develop from persistent HPV infection and potentially progress to cancer over many years if left untreated. Diagnosis involves Pap smear, colposcopy, and biopsy. Staging uses the FIGO system and determines treatment, which may include surgery, radiation therapy, or chemoradiation depending on the stage. The choice of treatment also considers the patient's age and fitness.