Downloaded 84 times
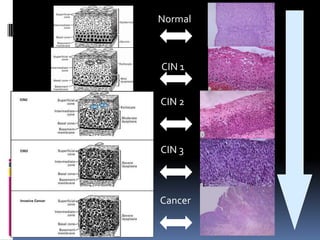
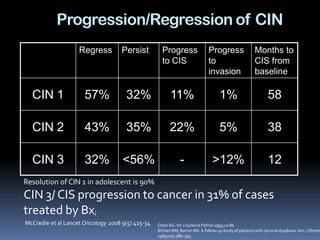
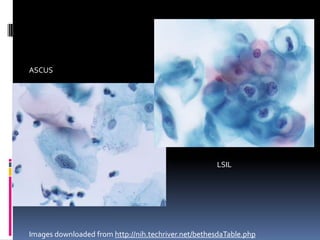











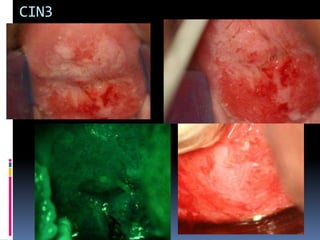

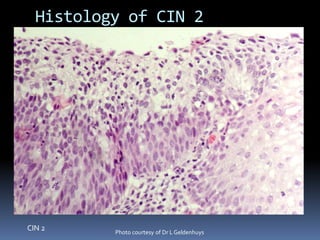
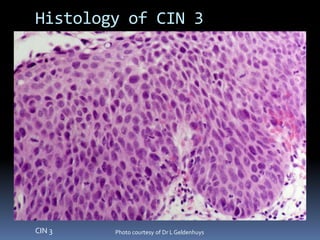



1) Differentiating between high grade (CIN 2/3) and low grade (CIN 1) cervical lesions is important for treatment decisions. 2) Colposcopic features that suggest high grade lesions include coarse mosaicism, irregular blood vessels, thick opaque white epithelium, well-demarcated ridges, and papillary configurations with sharp borders. 3) Low grade lesions typically have features like a transient whitening with acetic acid, fine punctation, ill-defined margins, and peripheral or small sizes.