Download as PDF, PPTX

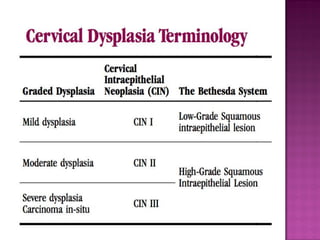
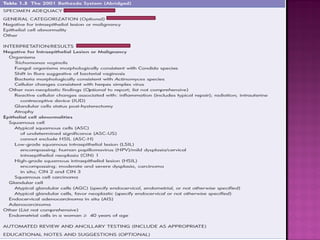
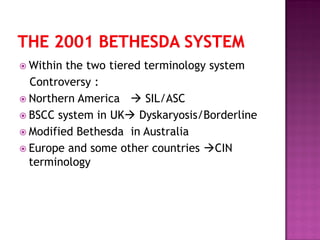

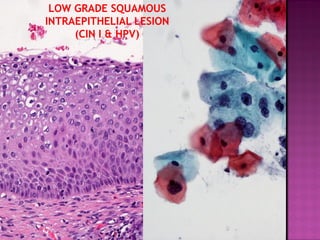

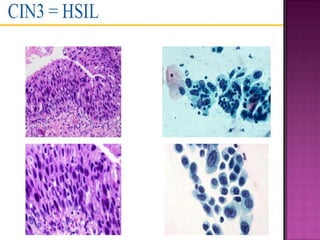
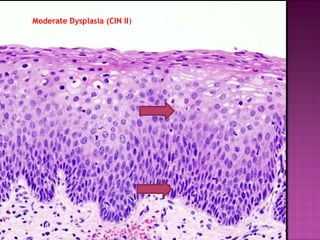
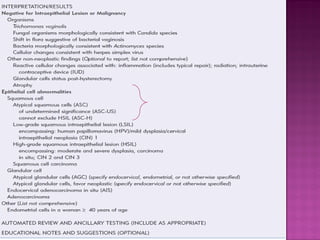


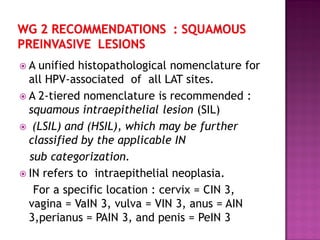
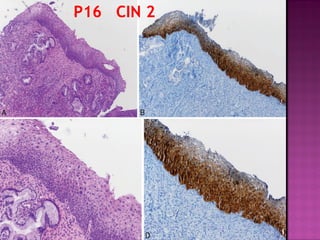


This document discusses the terminology used for preinvasive cervical lesions. It begins with definitions of dysplasia and provides a historical review of terminology, including carcinoma in situ (CIS) and cervical intraepithelial neoplasia (CIN). It then describes the 2001 Bethesda System for cervical cytology reporting and the Lower Anogenital Squamous Terminology (LAST) project. The LAST project aimed to create a unified histopathological nomenclature for HPV-associated preinvasive lesions across anatomical sites, recommending a two-tiered system of low-grade squamous intraepithelial lesions (LSIL) and high-grade squamous intraepithelial lesions (HSIL).



































































![ANIMAL_CELL_,_TISSUE_AND_ORGAN_CULTURE[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/animalcelltissueandorganculture1-260204172026-4462b440-thumbnail.jpg?width=640&height=640&fit=bounds)















![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)

