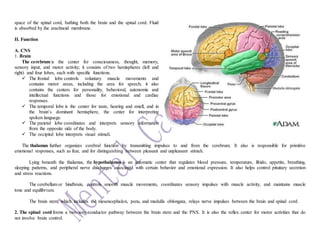
This document is a comprehensive case study on schizophrenia involving a 35-year-old male patient, Mr. MP, who displays significant symptoms of the disorder, including lack of cooperation and withdrawal from interactions. It covers patient assessments, clinical manifestations, treatment options such as antipsychotic medications, and nursing interventions aimed at promoting socialization and ensuring safety during management. Additionally, it includes details on the anatomical and physiological aspects of the neurological system relevant to the patient's condition.








![Psychiatry history taking and mental state examination [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/psychiatryhistorytakingandmentalstateexaminationautosaved-200909142851-thumbnail.jpg?width=640&height=640&fit=bounds)


































































































