Downloaded 279 times
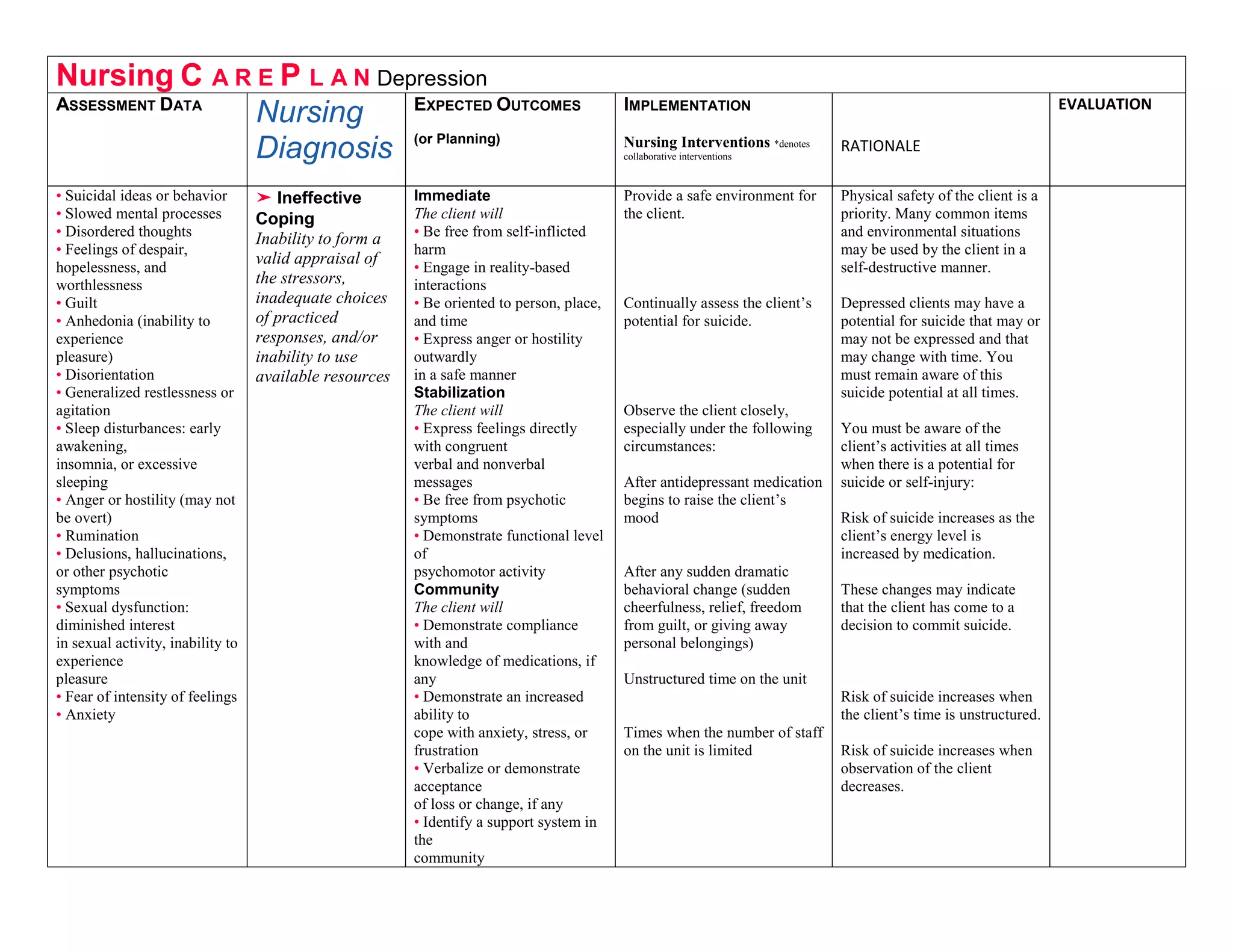

This nursing care plan outlines the assessment data, expected outcomes, nursing diagnosis, and implementation strategies for a client experiencing depression. The client presents with symptoms including suicidal thoughts, slowed mental processes, disordered thoughts, feelings of despair and worthlessness, and sleep disturbances. The nursing diagnosis is ineffective coping. Expected immediate outcomes are for the client to be free from self-harm, engage in reality-based interactions, and be oriented. Stabilization outcomes include expressing feelings directly and being free from psychotic symptoms. Community outcomes are medication compliance if prescribed, increased ability to cope with stress, and identifying a support system. Nursing interventions include providing a safe environment, continually assessing suicide risk, closely observing the client during medication changes or behavioral changes,