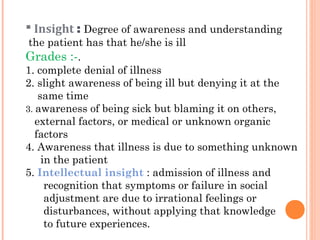
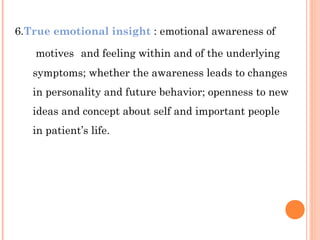
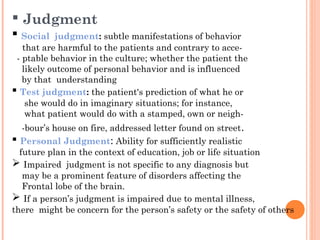


The document discusses the components and purpose of a mental status examination (MSE). A MSE is used to assess a patient's mental state and behavior through objective observations and subjective reports. It provides information for diagnosis, treatment assessment, and comparison over time. The key components of a MSE include appearance, behavior, speech, mood, thought processes, thought content, cognition, insight, and judgment. A MSE allows clinicians to evaluate changes in a patient's condition.

![Psychiatry history taking and mental state examination [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/psychiatryhistorytakingandmentalstateexaminationautosaved-200909142851-thumbnail.jpg?width=640&height=640&fit=bounds)





























![PRESENTATION ON MHN UNIT 2 PPTX[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonmhnunit2pptx1-250906125029-cec4c130-thumbnail.jpg?width=640&height=640&fit=bounds)
![MENTAL STATUS EAMINATION[MSE] for undergraduates (Psych)](https://cdn.slidesharecdn.com/ss_thumbnails/mentalstatuseaminationmseforundergraduatespsych-250812021929-dd507eb8-thumbnail.jpg?width=640&height=640&fit=bounds)


































