Download as PDF, PPTX


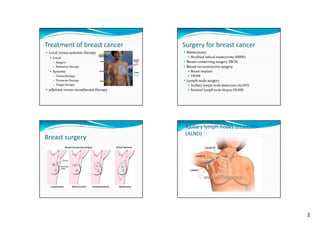
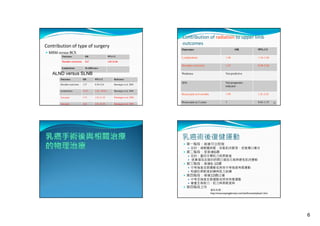
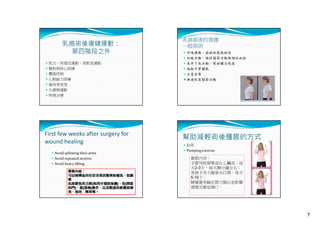
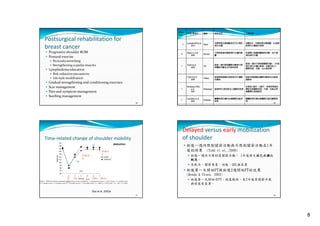

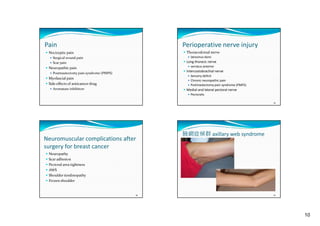
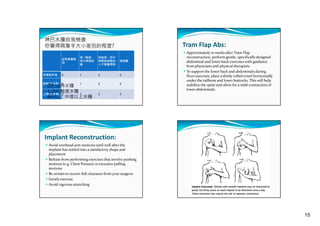
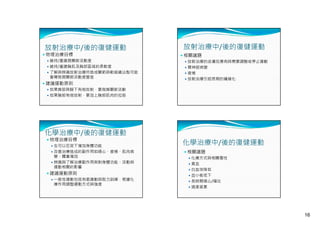

This document summarizes treatment for breast cancer, including surgery, radiation therapy, chemotherapy, hormone therapy, and targeted therapy. It discusses different types of breast surgery including mastectomy, breast-conserving surgery, lymph node surgery, and breast reconstruction. It also covers common side effects of chemotherapy and hormone therapy. Physical therapy exercises for breast cancer recovery are proposed in four phases focusing on range of motion, strength, flexibility, and endurance.



































































![20131013 03 黃曉峰_安寧緩和照護團隊之決策與溝通 [相容模式]](https://cdn.slidesharecdn.com/ss_thumbnails/2013101303-131030031643-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![20131013 02 翁益強_安寧緩和照護之法律與倫理講義 [相容模式]](https://cdn.slidesharecdn.com/ss_thumbnails/2013101302-131030031642-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
