Downloaded 16 times
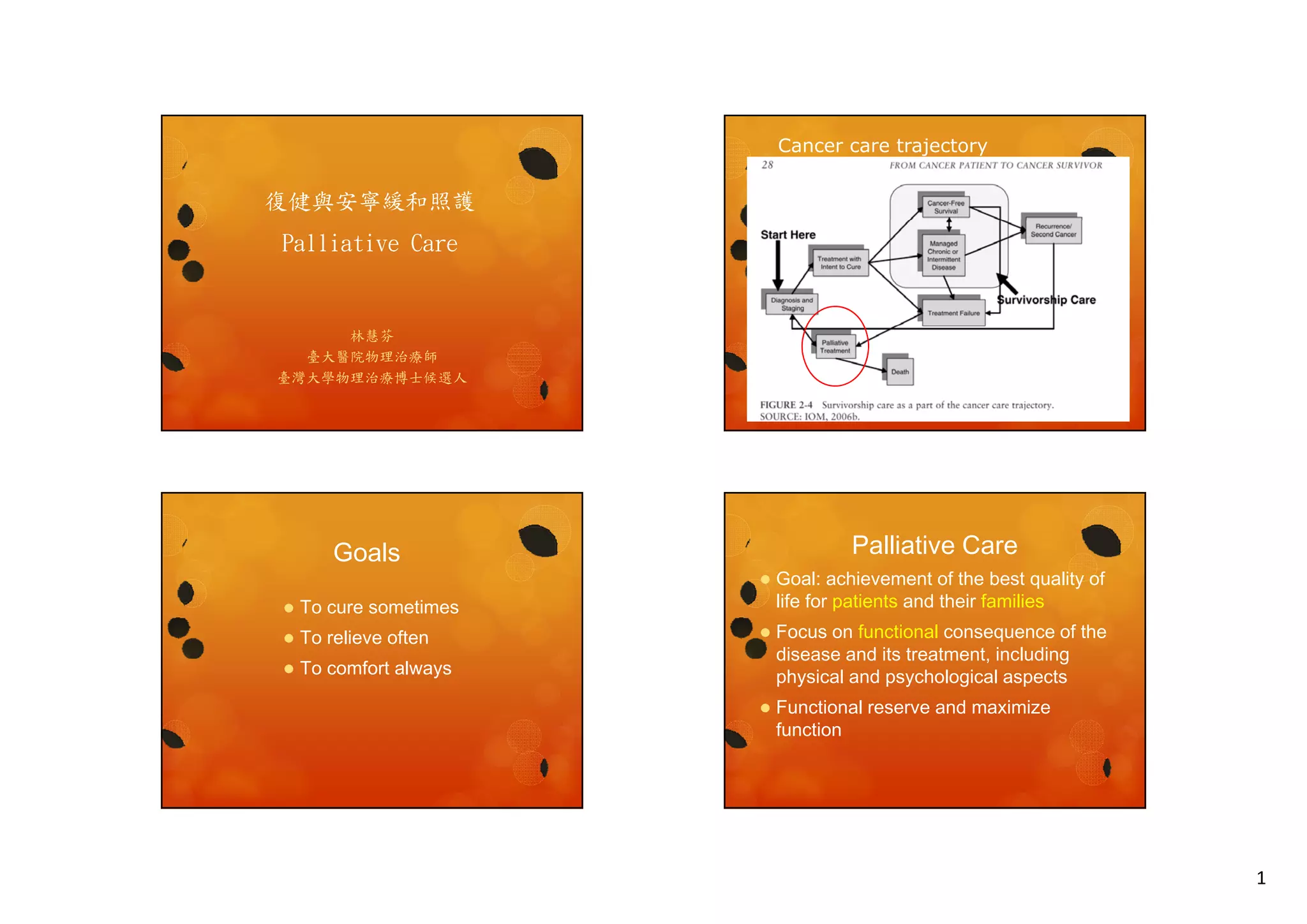
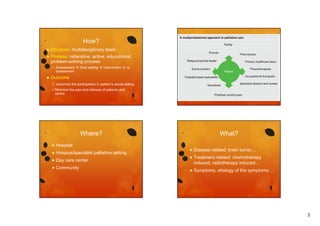






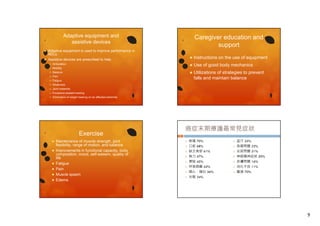






The document discusses palliative care, which aims to relieve suffering and improve quality of life for patients with serious illnesses. It provides an overview of palliative care goals, processes, interventions, symptoms addressed, and tools used to assess patients' physical functioning and set functional goals. The document also outlines examples of physical therapy interventions for common issues like pain, dyspnea, and fatigue in cancer patients.


















































![20131013 03 黃曉峰_安寧緩和照護團隊之決策與溝通 [相容模式]](https://cdn.slidesharecdn.com/ss_thumbnails/2013101303-131030031643-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![20131013 02 翁益強_安寧緩和照護之法律與倫理講義 [相容模式]](https://cdn.slidesharecdn.com/ss_thumbnails/2013101302-131030031642-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


