Download as PDF, PPTX



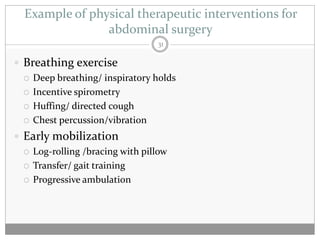
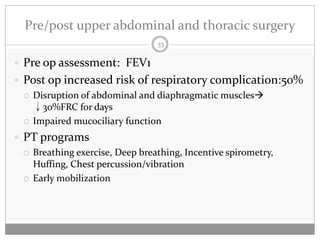
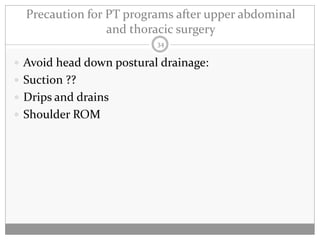
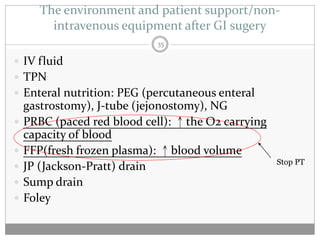
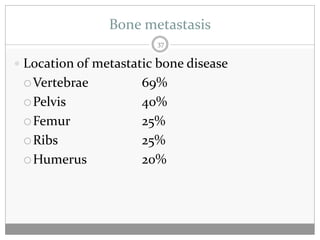
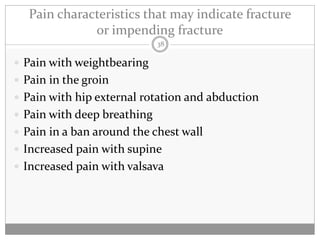

The document discusses physical therapy interventions for cancer patients after surgery, focusing on early mobilization, lung hygiene exercises, and specific rehabilitation programs for common cancer types like breast cancer, lung cancer, and gastrointestinal cancers. Post-surgery goals include preventing complications, improving range of motion, and managing symptoms like pain, breathlessness, and bone metastasis. Precautions and considerations for different surgeries are also outlined.


































![Physiotherapy in pulmonary_surgery[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarysurgery1-230705093621-2b78f958-thumbnail.jpg?width=640&height=640&fit=bounds)
















![20131013 03 黃曉峰_安寧緩和照護團隊之決策與溝通 [相容模式]](https://cdn.slidesharecdn.com/ss_thumbnails/2013101303-131030031643-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![20131013 02 翁益強_安寧緩和照護之法律與倫理講義 [相容模式]](https://cdn.slidesharecdn.com/ss_thumbnails/2013101302-131030031642-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)














