Downloaded 68 times

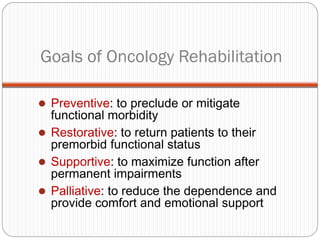
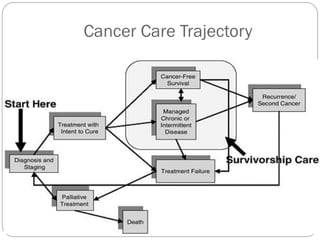
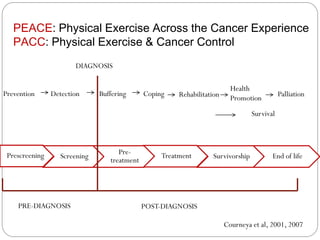
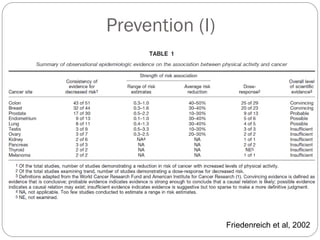
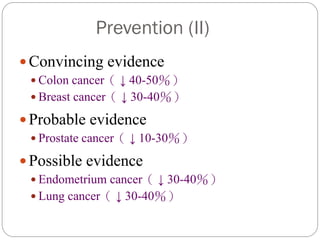
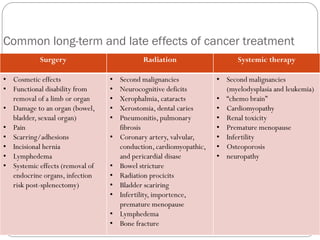
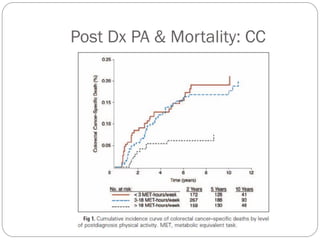
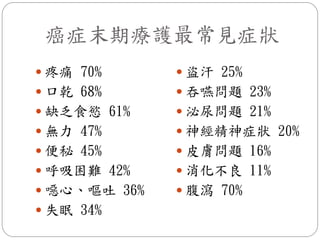

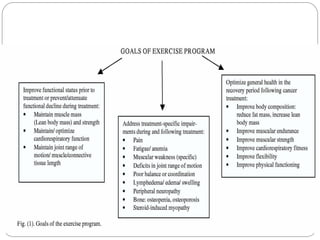
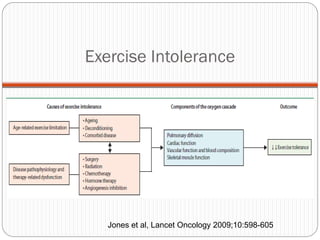
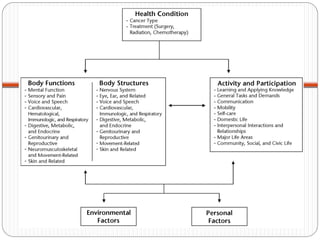
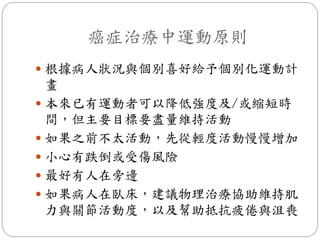
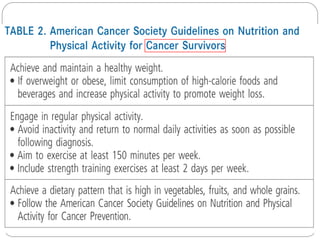
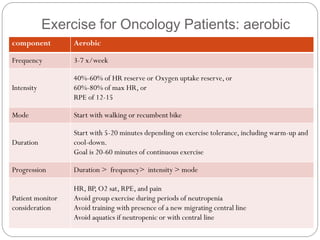
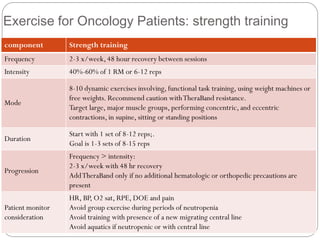

The document discusses exercise for cancer patients across the cancer care trajectory. It covers goals of cancer rehabilitation including prevention, restoration, support, and palliation. It then discusses exercise for prevention, detection, coping with treatment, rehabilitation after treatment, survival, health promotion, and palliation. Specific benefits of exercise discussed include reducing cancer risk and recurrence, managing treatment side effects, and improving physical and psychological well-being.






































































![20131013 03 黃曉峰_安寧緩和照護團隊之決策與溝通 [相容模式]](https://cdn.slidesharecdn.com/ss_thumbnails/2013101303-131030031643-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![20131013 02 翁益強_安寧緩和照護之法律與倫理講義 [相容模式]](https://cdn.slidesharecdn.com/ss_thumbnails/2013101302-131030031642-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)















