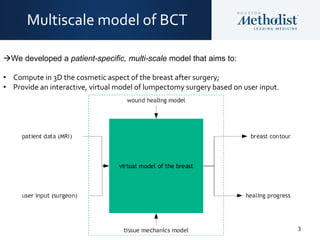
This document discusses a predictive multiscale model for breast conserving therapy that was developed to:
1) Compute the cosmetic outcome of the breast after surgery in 3D.
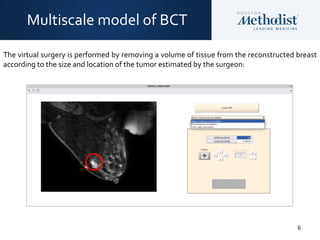
2) Provide an interactive virtual model of lumpectomy surgery based on user input.
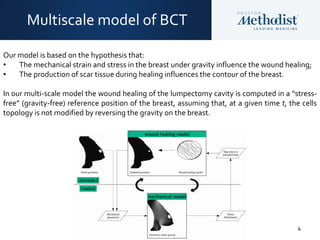
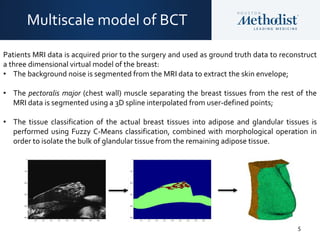
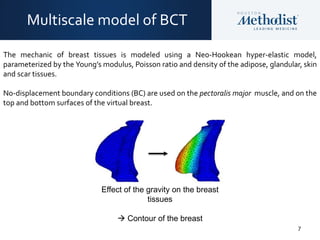
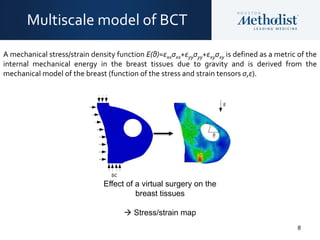
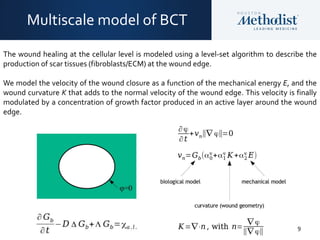
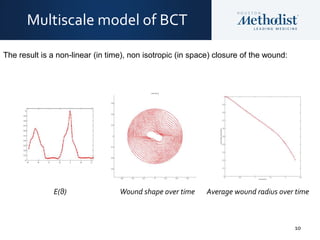
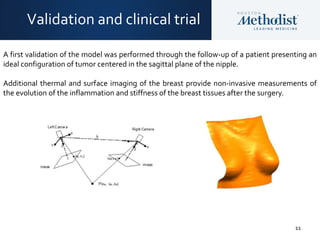
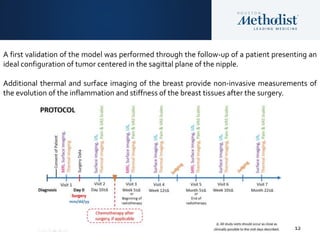
The model hypothesizes that mechanical strain and stress from gravity influence wound healing, and scar tissue production during healing influences the breast contour. It uses patient MRI data and models tissue mechanics and wound healing at the cellular level to simulate breast shape over time. Validation with patient data helped optimize key parameters impacting cosmetic results.