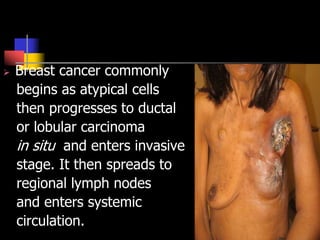
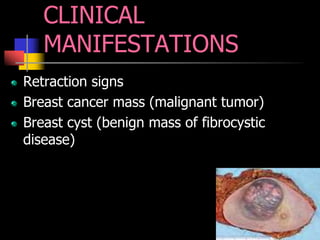
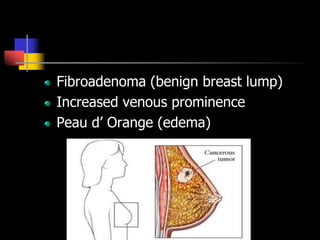
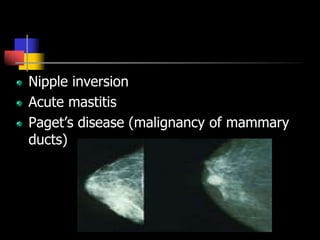
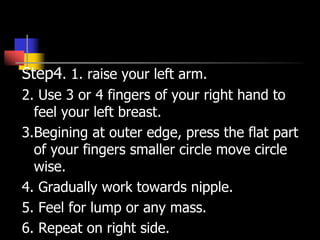
This document provides information about breast cancer including its definition, anatomy, risk factors, etiological factors, pathophysiology, clinical manifestations, stages, diagnostic tests, treatment, management, and nursing care. It discusses how breast cancer begins in the ductal or lobular cells and can spread through the lymphatic system and bloodstream. Risk factors include family history, obesity, lack of breastfeeding. Treatment may involve surgery, radiation, chemotherapy, hormone therapy and pain management. Nursing care focuses on education, managing anxiety and pain, and promoting healthy coping.