Download to read offline



























![35
The concentration of Na+
in ICF,
([Na+
]i) is 10 mmol/L.
The concentration of Na+
in ECF,
([Na+
]e) is 130~150 mmol/L.
](https://image.slidesharecdn.com/2normalmetabolismofwaterandsodium-190401175424/75/2-normalmetabolismofwaterandsodium-35-2048.jpg)
















![52
renal
blood flow
[Na+] in
macula densa
excitement of
sympathetic nerve
renin release from the
juxtaglomerular cells
increase of angiotensin II
releases
[K+], [Na+]
blood flow in plasma
aldosterone secretion from
adrenal cortex
Na+ reaborption in
renal tubules
K+ and H+ excretion
from kidneys](https://image.slidesharecdn.com/2normalmetabolismofwaterandsodium-190401175424/75/2-normalmetabolismofwaterandsodium-52-2048.jpg)






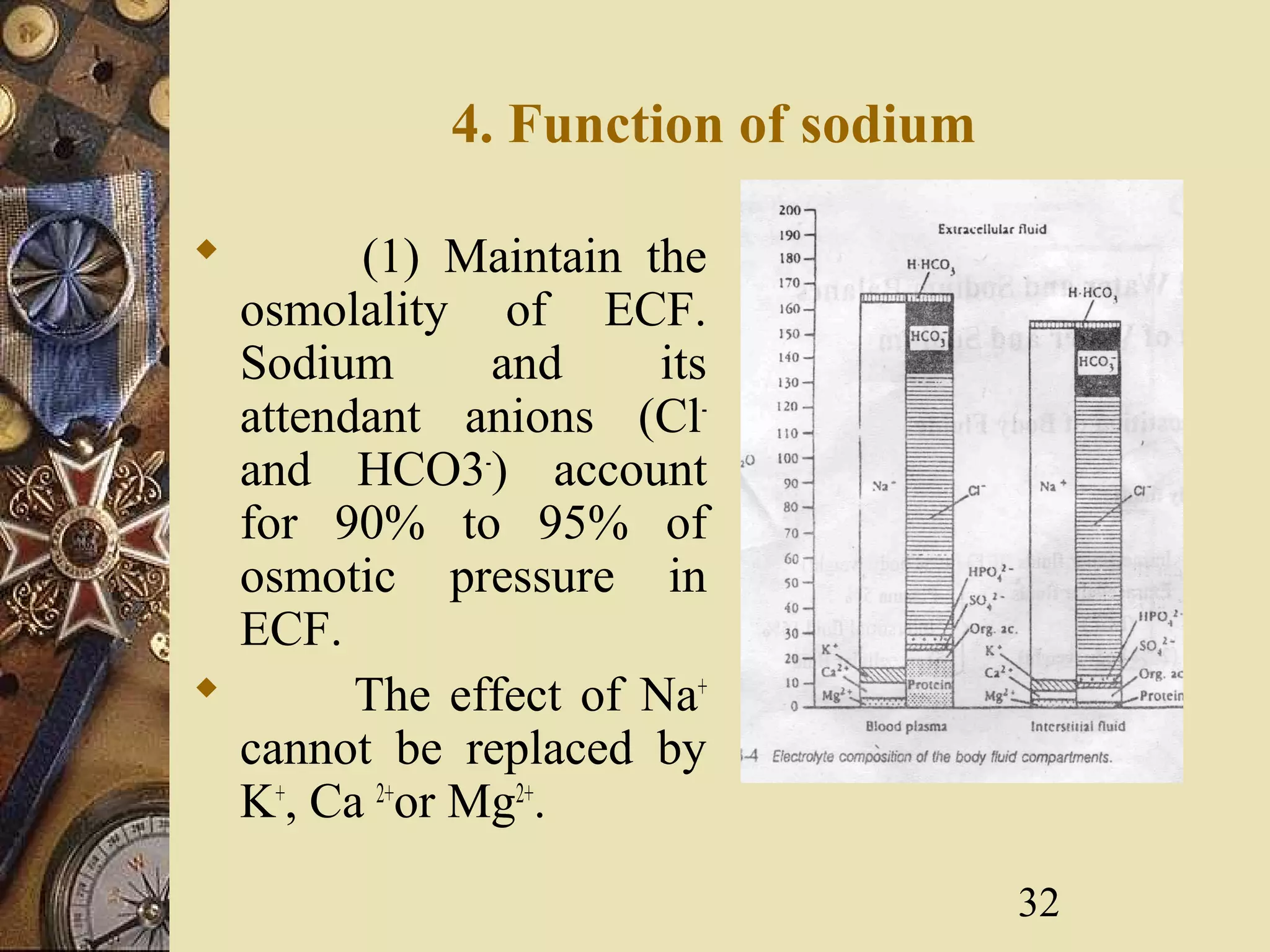
This document discusses the normal metabolism of water and sodium in the body. It covers topics such as the distribution and composition of body fluids, osmotic pressure, and the regulation of water and sodium levels. Water intake and loss must be balanced to maintain homeostasis. The kidneys play an important role in regulating sodium balance by excreting more or less sodium depending on intake levels. Hormones like ADH and aldosterone also help regulate water and sodium metabolism in the body.























































































