Downloaded 114 times
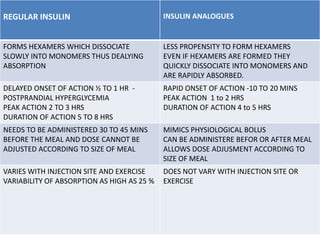

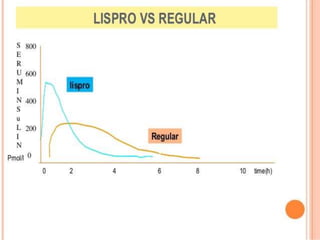
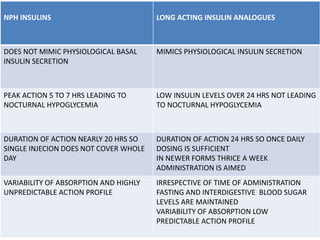
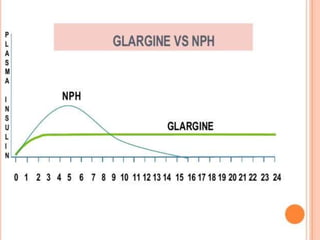




Insulin analogues are genetically engineered versions of human insulin that are designed to more closely mimic the body's natural insulin secretion. Short-acting analogues like lispro and aspart have a faster onset of action than regular insulin, allowing for more flexibility in dosing around meals. Long-acting analogues like glargine and degludec aim to provide a steady basal insulin level throughout the day without peaks, reducing the risk of nocturnal hypoglycemia. While insulin analogues provide benefits over regular insulin in terms of better glycemic control and reduced side effects, their higher cost is still a limitation to their use.







































![diabetes.pptxgtgthtgtgtgthyjiulp'][pp0ppp](https://cdn.slidesharecdn.com/ss_thumbnails/diabetes-250824142109-beeb6b11-thumbnail.jpg?width=640&height=640&fit=bounds)















































