Download to read offline
















This document presents a case study of a 50-year-old female patient who presented with loose stools for 2 days. Her condition did not improve with initial treatment and her diarrhea increased to 20-30 episodes per day. Laboratory tests found Entamoeba histolytica cysts in her stool. Despite treatment with antibiotics, antiamoebic medications, and loperamide, her condition continued to worsen with increased diarrhea episodes. A CT scan showed a simple liver cyst but no other abnormalities. The case is presented for discussion as the patient's condition has not responded to treatment.
Introduction to a clinical case involving a 50-year-old female patient with diarrhea. Details include patient history, symptoms, and personal background. The patient experiences loose stools (15-20 episodes) without fever. Examination shows mild dehydration, consistent vital signs, and a general assessment.
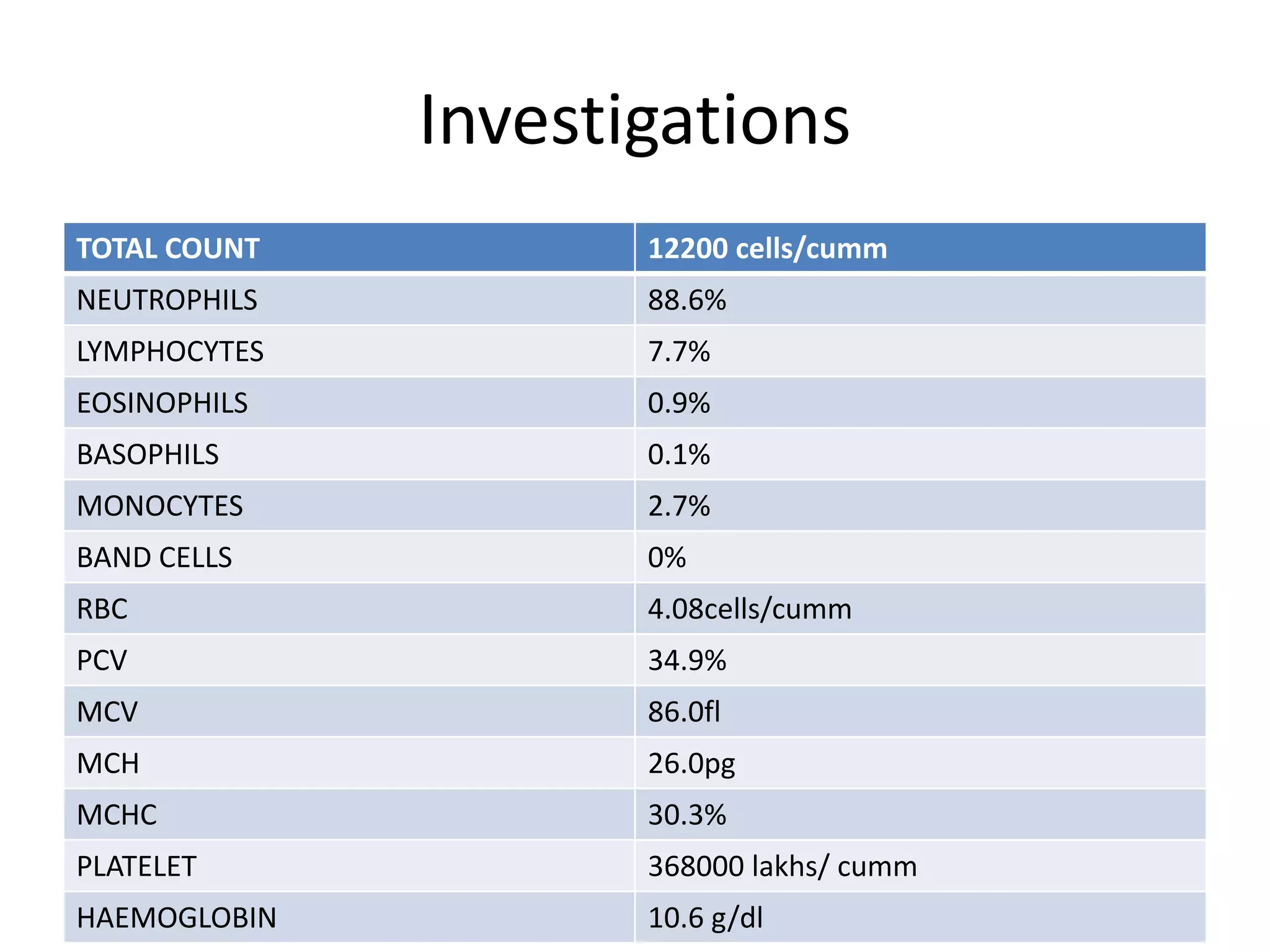
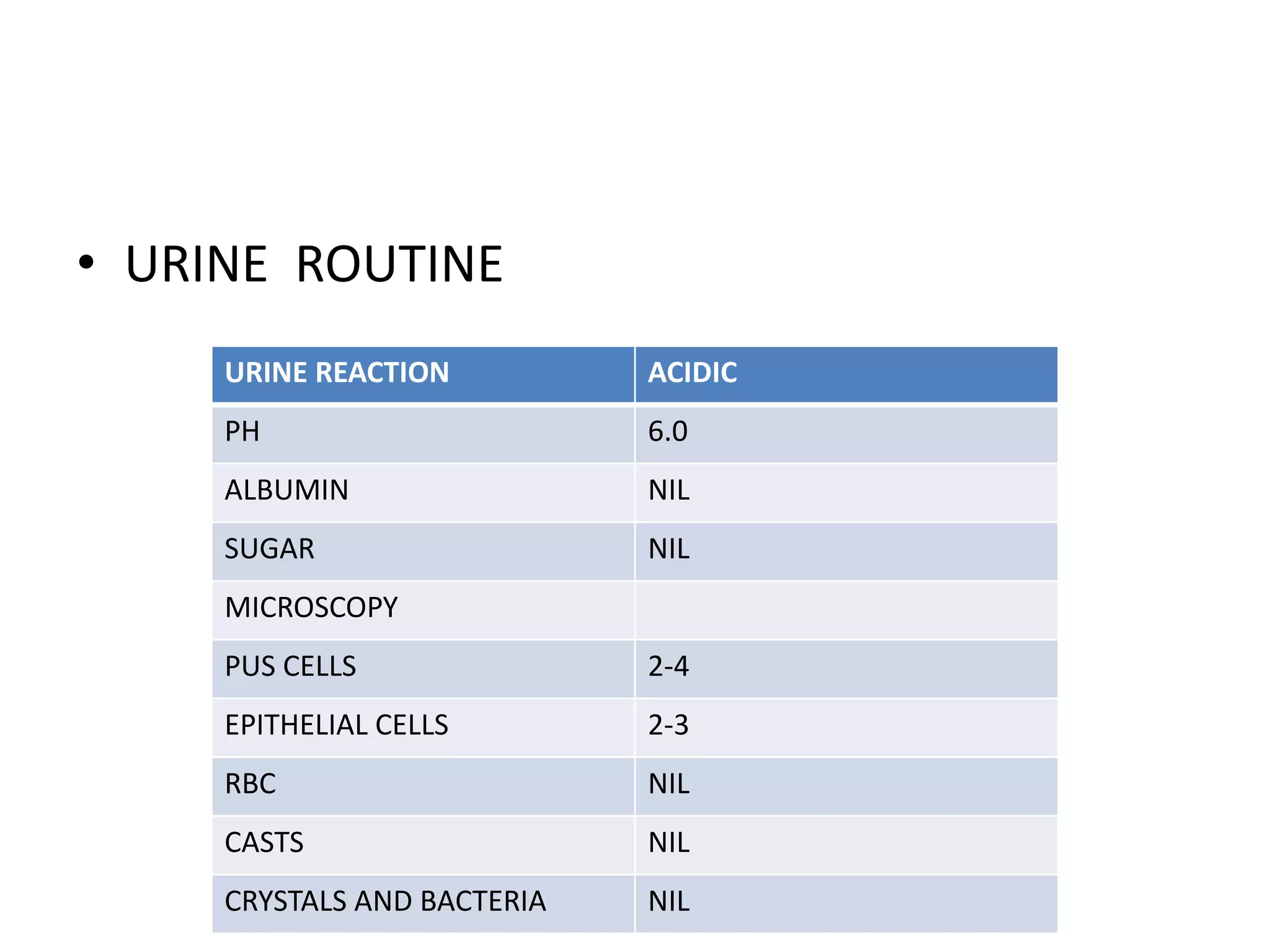
Blood tests indicating leukocytosis with high neutrophils, normal renal function, and liver function tests within normal limits. Urine analysis shows no significant abnormalities.
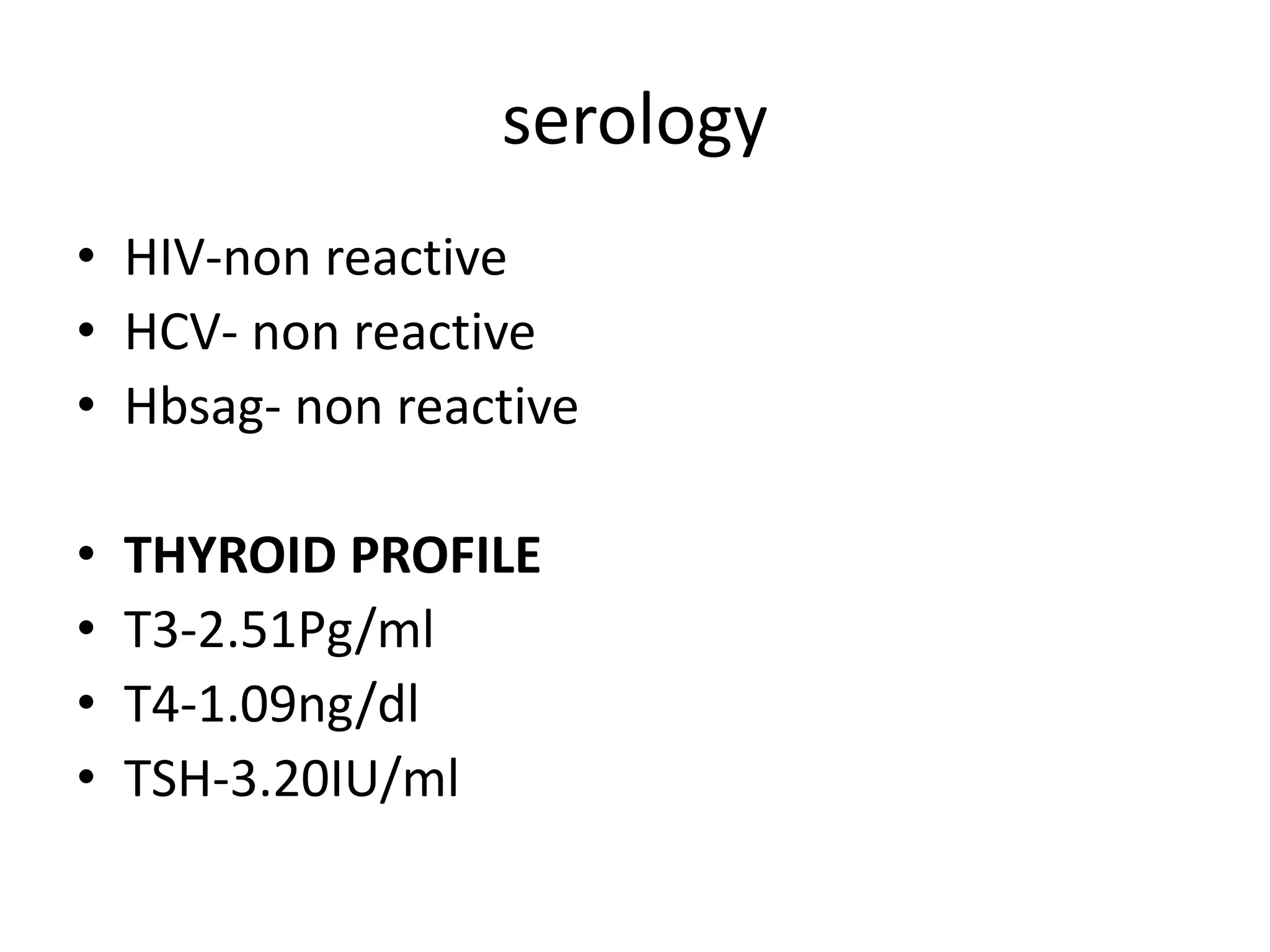
Negative serology results and stool examination positive for Entamoeba histolytica cysts; abdominal ultrasound reveals no significant abnormality.
Initial treatment included IV fluids and anti-diarrheal medications. Despite treatment, diarrhea worsened, requiring further intervention and discussion of case.























































































