Downloaded 270 times
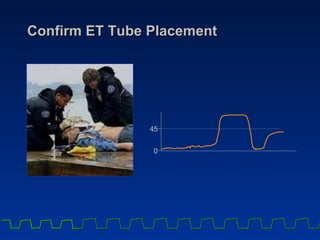
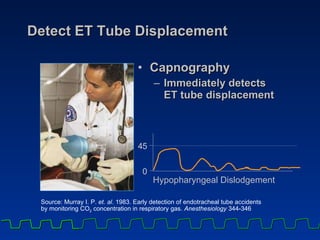
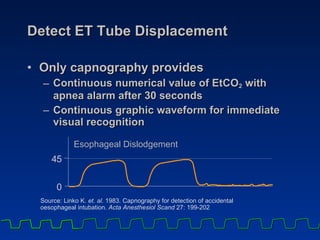
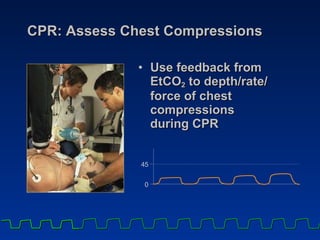
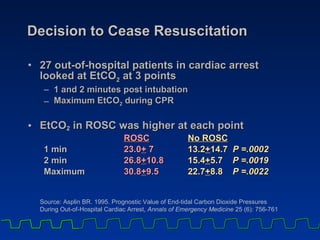
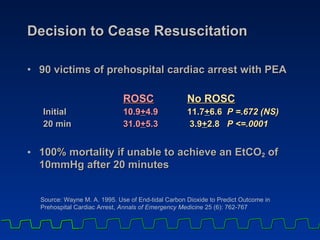

Capnography can be used to summarize 3 key applications for intubated patients: 1) It can confirm correct endotracheal tube placement and detect displacement. Characteristic waveforms indicate proper vs displaced placement. 2) During CPR, it can assess the effectiveness of chest compressions by correlating end-tidal CO2 levels with cardiac output and blood flow. 3) It provides an early indicator of return of spontaneous circulation through a rapid rise in CO2 levels, earlier than other signs like pulse or blood pressure. It also aids the decision to cease resuscitation efforts based on CO2 levels.


























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















