Download as PDF, PPTX

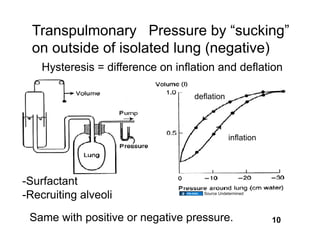
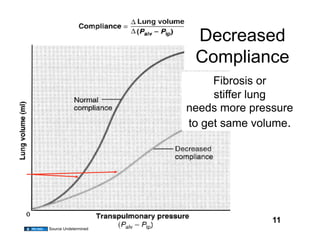
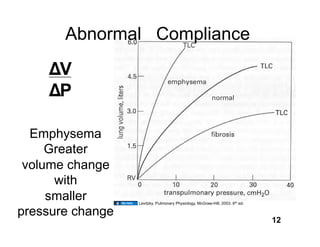
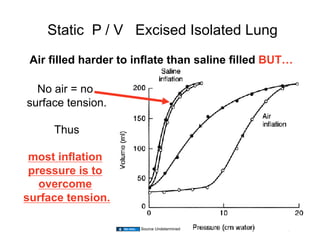
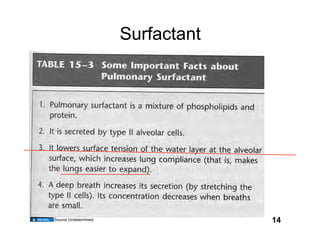
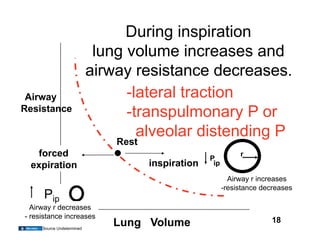
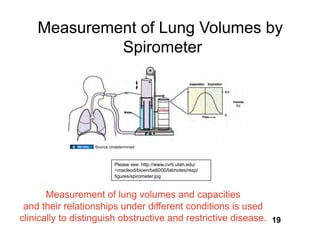
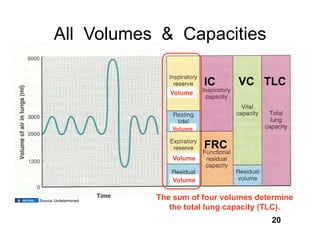
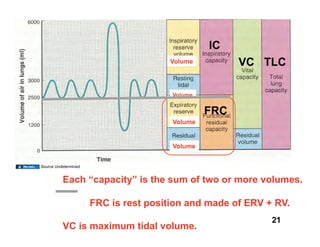
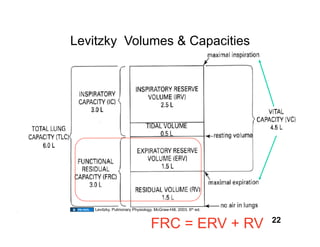
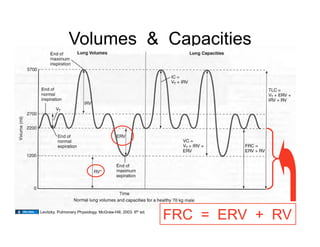
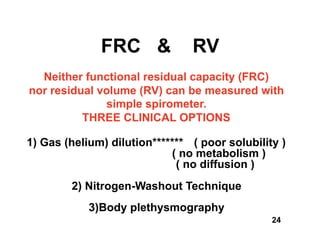
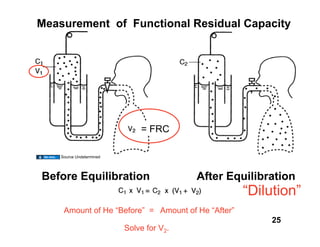
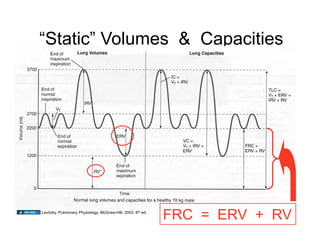




The document discusses respiratory mechanics, particularly the mechanics of ventilation and various lung volumes and capacities, citing the work of Louis D'Alecy and referring to his educational material. It emphasizes the importance of tidal volume, intrapleural pressure, lung compliance, and airway resistance, as well as methods to measure lung volumes clinically. Additionally, it outlines copyright permissions regarding the use and adaptation of the material, and includes various sources for further reference.
































































































