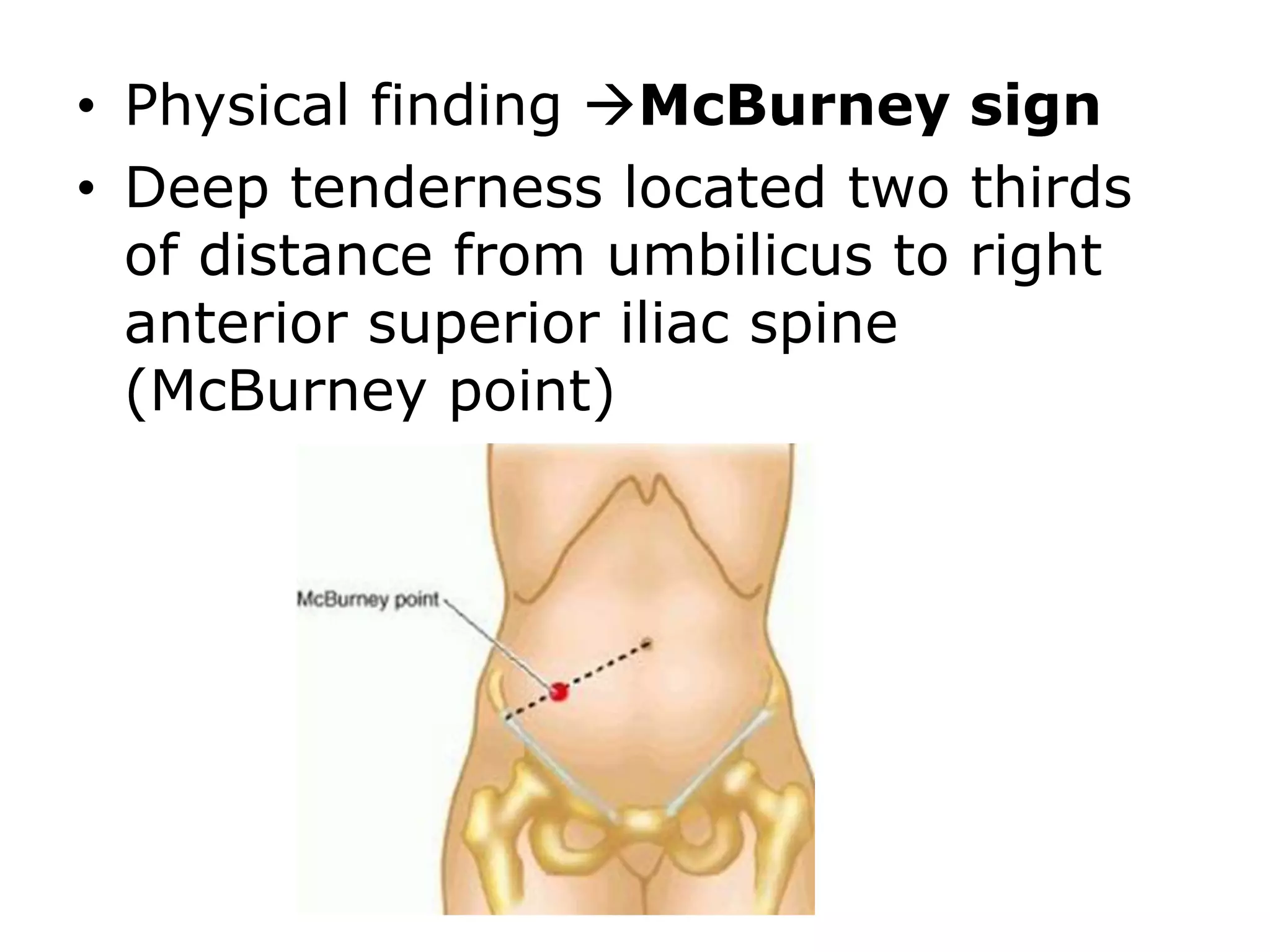
Acute appendicitis is caused by obstruction of the appendix lumen, usually by a fecalith, leading to bacterial overgrowth and inflammation. It most commonly affects adolescents and young adults. Early symptoms include periumbilical pain that moves to the lower right abdomen, nausea, vomiting, and fever. On physical exam, tenderness is found at McBurney's point. Without treatment, complications can arise like perforation or abscess. The most common tumor of the appendix is carcinoid tumor, while other rare tumors can cause appendicitis-like symptoms.